Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, USA.
PLoS Med. 2013 Aug;10(8):e1001502. doi: 10.1371/journal.pmed.1001502. Epub 2013 Aug 20.
Neonatal infections cause a significant proportion of deaths in the first week of life, yet little is known about risk factors and pathways of transmission for early-onset neonatal sepsis globally. We aimed to estimate the risk of neonatal infection (excluding sexually transmitted diseases [STDs] or congenital infections) in the first seven days of life among newborns of mothers with bacterial infection or colonization during the intrapartum period.
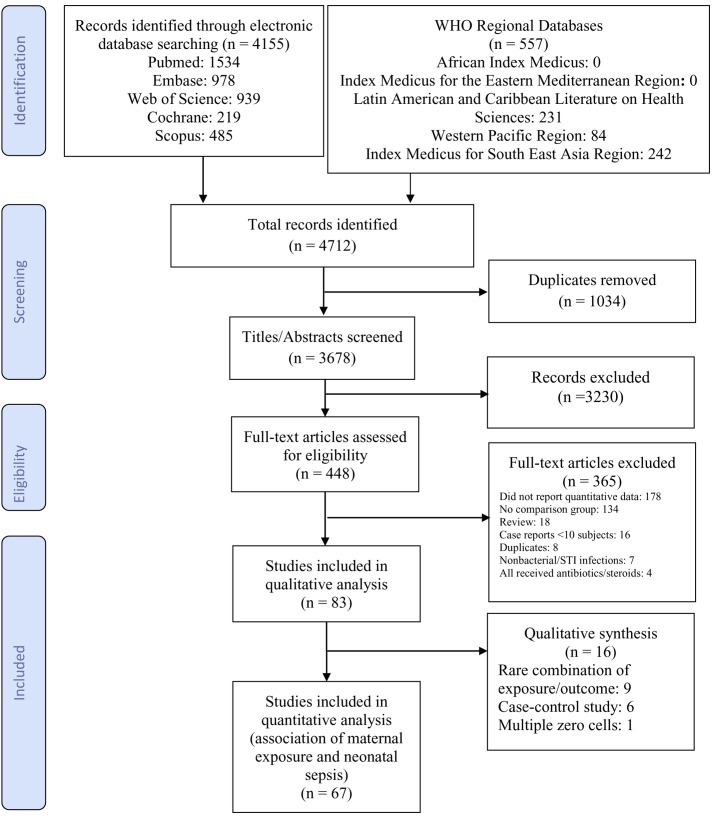
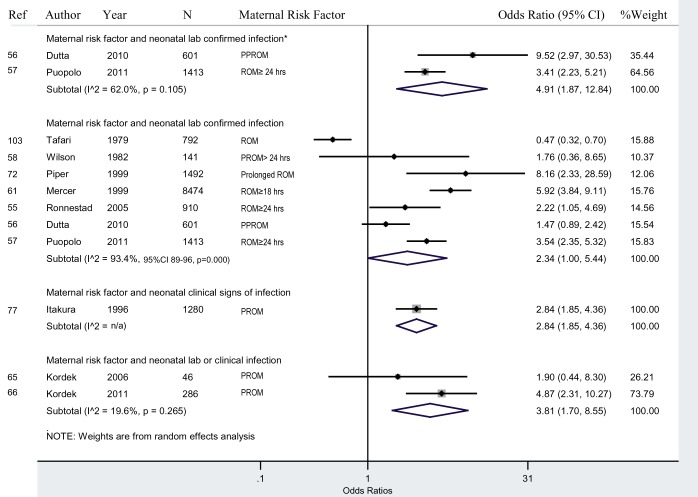
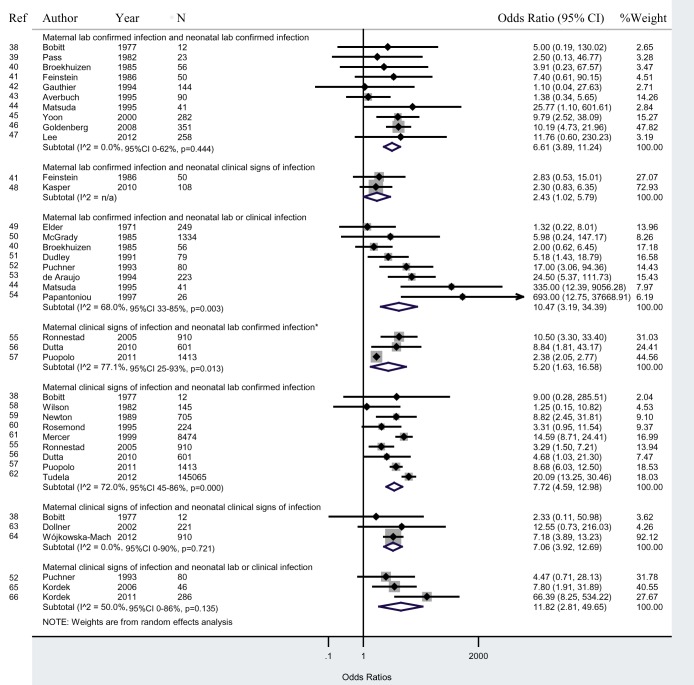
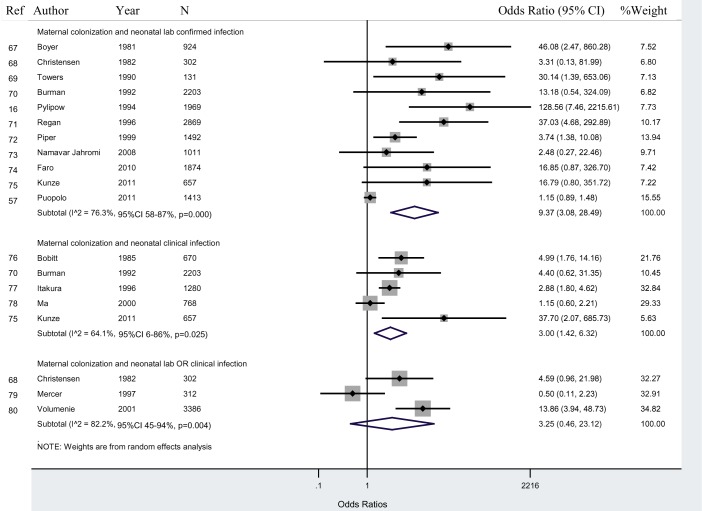
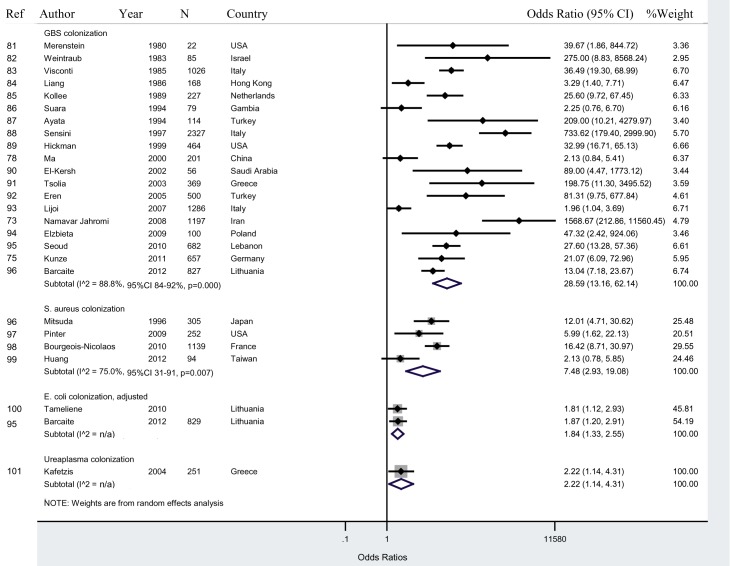
We searched PubMed, Embase, Scopus, Web of Science, Cochrane Library, and the World Health Organization Regional Databases for studies of maternal infection, vertical transmission, and neonatal infection published from January 1, 1960 to March 30, 2013. Studies were included that reported effect measures on the risk of neonatal infection among newborns exposed to maternal infection. Random effects meta-analyses were used to pool data and calculate the odds ratio estimates of risk of infection. Eighty-three studies met the inclusion criteria. Seven studies (8.4%) were from high neonatal mortality settings. Considerable heterogeneity existed between studies given the various definitions of laboratory-confirmed and clinical signs of infection, as well as for colonization and risk factors. The odds ratio for neonatal lab-confirmed infection among newborns of mothers with lab-confirmed infection was 6.6 (95% CI 3.9-11.2). Newborns of mothers with colonization had a 9.4 (95% CI 3.1-28.5) times higher odds of lab-confirmed infection than newborns of non-colonized mothers. Newborns of mothers with risk factors for infection (defined as prelabour rupture of membranes [PROM], preterm <37 weeks PROM, and prolonged ROM) had a 2.3 (95% CI 1.0-5.4) times higher odds of infection than newborns of mothers without risk factors.
Neonatal infection in the first week of life is associated with maternal infection and colonization. High-quality studies, particularly from settings with high neonatal mortality, are needed to determine whether targeting treatment of maternal infections or colonization, and/or prophylactic antibiotic treatment of newborns of high risk mothers, may prevent a significant proportion of early-onset neonatal sepsis. Please see later in the article for the Editors' Summary.
新生儿感染是导致生命最初一周内死亡的一个重要原因,但目前全球对于早发型新生儿败血症的发病因素和传播途径知之甚少。我们旨在评估分娩期母亲感染或定植细菌的新生儿在生命最初 7 天内发生感染(不包括性传播疾病[STD]或先天性感染)的风险。
我们检索了 1960 年 1 月 1 日至 2013 年 3 月 30 日期间发表的关于母亲感染、垂直传播和新生儿感染的PubMed、Embase、Scopus、Web of Science、Cochrane 图书馆和世界卫生组织区域数据库的研究。纳入了报告暴露于母亲感染的新生儿感染风险的研究。采用随机效应荟萃分析对数据进行合并,并计算风险比的估计值。83 项研究符合纳入标准。其中 7 项研究(8.4%)来自新生儿死亡率较高的地区。由于实验室确认感染和临床感染体征的定义以及定植和危险因素的不同,研究之间存在很大的异质性。母亲实验室确认感染的新生儿发生实验室确认感染的比值比为 6.6(95%CI 3.9-11.2)。母亲定植的新生儿发生实验室确认感染的比值比为 9.4(95%CI 3.1-28.5),而非定植母亲的新生儿发生实验室确认感染的比值比高。具有感染危险因素(定义为胎膜早破[PROM]、早产<37 周胎膜早破和胎膜早破时间延长)的母亲的新生儿发生感染的比值比为 2.3(95%CI 1.0-5.4),高于无危险因素母亲的新生儿。
新生儿在生命最初一周内发生感染与母亲感染和定植有关。需要高质量的研究,特别是来自新生儿死亡率较高的地区,以确定是否针对治疗母亲感染或定植以及/或对高危母亲的新生儿进行预防性抗生素治疗,可能会预防很大一部分早发型新生儿败血症的发生。请稍后在文章中查看编辑总结。