Wuethrich Patrick Y, Thalmann George N, Studer Urs E, Burkhard Fiona C
University Department of Anaesthesiology and Pain Therapy, University Hospital, Berne, Berne, Switzerland.
PLoS One. 2013 Aug 19;8(8):e72873. doi: 10.1371/journal.pone.0072873. eCollection 2013.
A beneficial effect of regional anesthesia on cancer related outcome in various solid tumors has been proposed. The data on prostate cancer is conflicting and reports on long-term cancer specific survival are lacking.
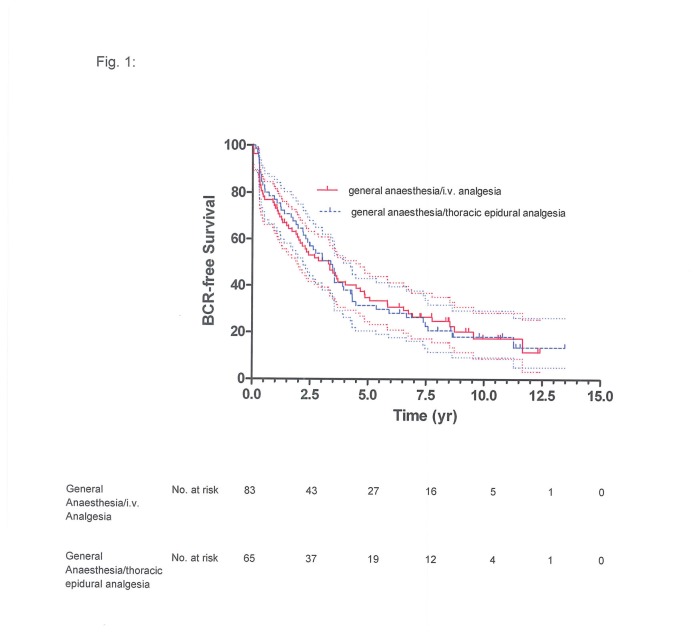
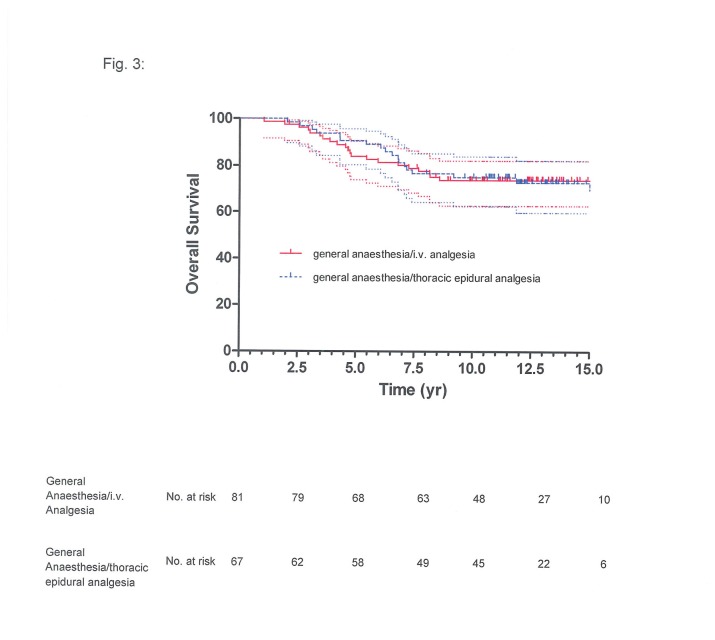
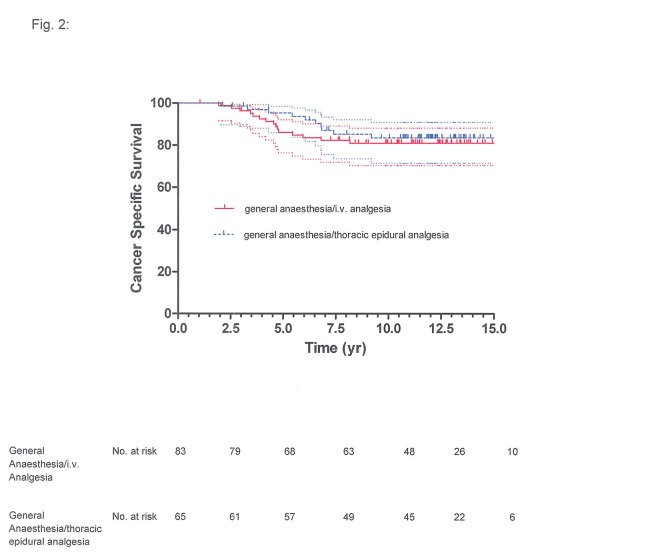
In a retrospective, single-center study, outcomes of 148 consecutive patients with locally advanced prostate cancer pT3/4 who underwent retropubic radical prostatectomy (RRP) with general anesthesia combined with intra- and postoperative epidural analgesia (n=67) or with postoperative ketorolac-morphine analgesia (n=81) were reviewed. The median observation time was 14.00 years (range 10.87-17.75 yrs). Biochemical recurrence (BCR)-free, local and distant recurrence-free, cancer-specific, and overall survival were estimated using the Kaplan-Meier technique. Multivariate Cox proportional-hazards regression models were used to analyze clinicopathologic variables associated with disease progression and death.
The survival estimates for BCR-free, local and distant recurrence-free, cancer-specific survival and overall survival did not differ between the two groups (P=0.64, P=0.75, P=0.18, P=0.32 and P=0.07). For both groups, higher preoperative PSA (hazard ratio (HR) 1.02, 95% confidence interval (CI) 1.01-1.02, P<0.0001), increased specimen Gleason score (HR 1.24, 95% CI 1.06-1.46, P=0.007) and positive nodal status (HR 1.66, 95% CI 1.03-2.67, P=0.04) were associated with higher risk of BCR. Increased specimen Gleason score predicted death from prostate cancer (HR 2.46, 95% CI 1.65-3.68, P<0.0001).
General anaesthesia combined with epidural analgesia did not reduce the risk of cancer progression or improve survival after RRP for prostate cancer in this group of patients at high risk for disease progression with a median observation time of 14.00 yrs.
区域麻醉对多种实体瘤的癌症相关预后具有有益作用,这一观点已被提出。关于前列腺癌的数据存在矛盾,且缺乏关于长期癌症特异性生存的报告。
在一项回顾性单中心研究中,对148例连续接受耻骨后根治性前列腺切除术(RRP)的局部晚期前列腺癌pT3/4患者的预后进行了评估,这些患者接受了全身麻醉联合术中和术后硬膜外镇痛(n = 67)或术后酮咯酸 - 吗啡镇痛(n = 81)。中位观察时间为14.00年(范围10.87 - 17.75年)。使用Kaplan - Meier技术估计无生化复发(BCR)、局部和远处无复发、癌症特异性和总生存率。多变量Cox比例风险回归模型用于分析与疾病进展和死亡相关的临床病理变量。
两组之间在无BCR、局部和远处无复发、癌症特异性生存和总生存的生存估计方面没有差异(P = 0.64,P = 0.75,P = 0.18,P = 0.32和P = 0.07)。对于两组,术前PSA升高(风险比(HR)1.02,95%置信区间(CI)1.01 - 1.02,P < 0.0001)、标本Gleason评分增加(HR 1.24,95% CI 1.06 - 1.46,P = 0.007)和淋巴结阳性状态(HR 1.66,95% CI 1.03 - 2.67,P = 0.04)与BCR风险较高相关。标本Gleason评分增加预示着前列腺癌死亡(HR 2.46,95% CI 1.65 - 3.68,P < 0.0001)。
对于这组疾病进展风险高、中位观察时间为14.00年的患者,全身麻醉联合硬膜外镇痛并不能降低前列腺癌RRP术后的癌症进展风险或提高生存率。