International Centre for Circulatory Health, National Heart and Lung Institute, London, United Kingdom.
International Centre for Circulatory Health, National Heart and Lung Institute, London, United Kingdom.
J Am Coll Cardiol. 2013 Dec 24;62(25):2406-2413. doi: 10.1016/j.jacc.2013.07.080. Epub 2013 Sep 4.
The goal of this study was to examine the impact of calculation-window duration on lifespan gain (as observed in trials) and on who gains most.
The landmark trials of biventricular pacing (cardiac resynchronization therapy [CRT]) typically ran for <1 device battery life, and they may therefore underestimate lifespan benefit over longer durations.
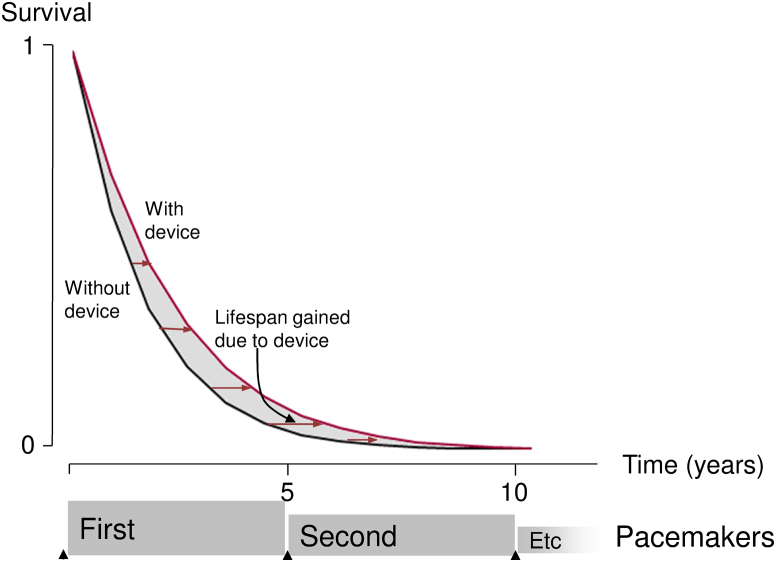
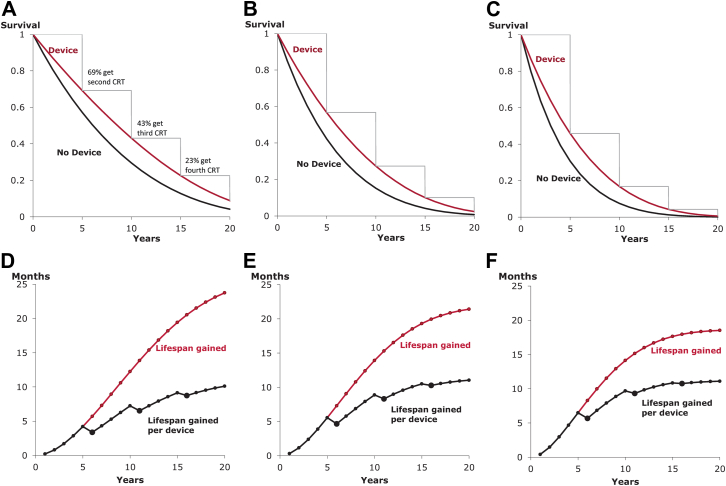
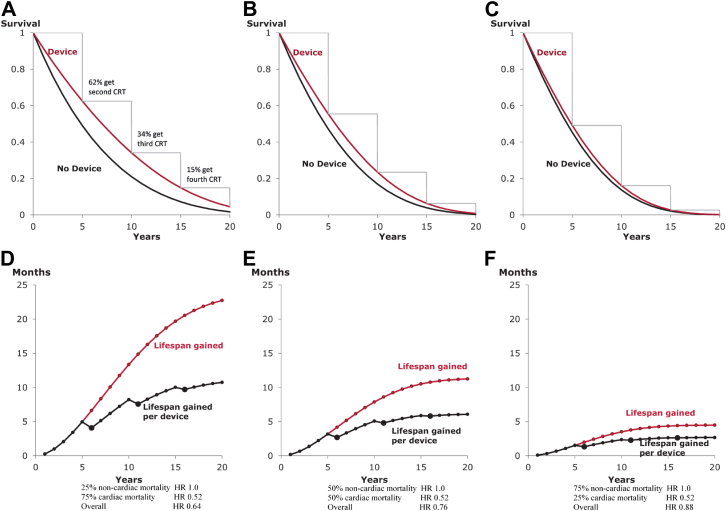
We conducted a meta-analysis of biventricular pacing trials to calculate lifespan gained: first, within the duration of randomized controlled trial data up to 2 years; second, over a 5-year typical battery life; and third, over >1 battery life. Importantly, we applied the Gompertz method for age-related increase in mortality from non-CRT-preventable causes.
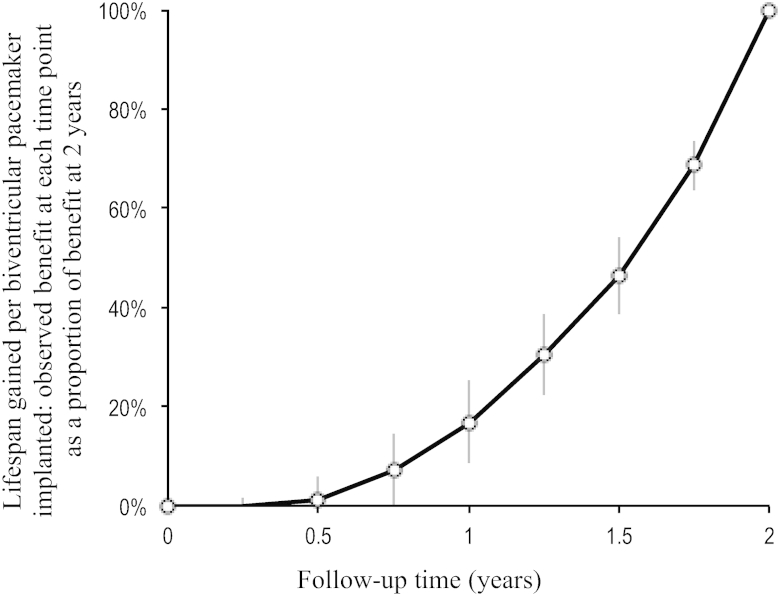
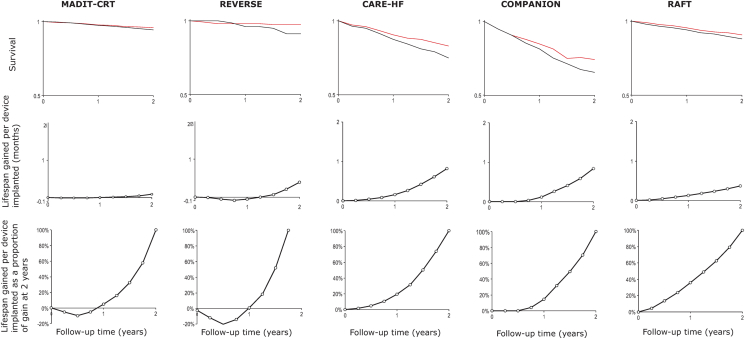
Five landmark trials (COMPANION [Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure], CARE-HF (CArdiac REsynchronization-Heart Failure), MADIT-CRT [Multicenter Automatic Defibrillator Implantation Trial With Cardiac Resynchronization Therapy], REVERSE [Resynchronization Reverses Remodeling in Systolic Left Ventricular Dysfunction], RAFT (Resynchronization-Defibrillation for Ambulatory Heart Failure)) provided data for 2 years (6,561 patients), with an average hazard ratio of 0.71. Lifespan gained across all trials increased nonlinearly with time from 0.1 month at 1 year, to 0.5 month at 2 years, and a projected 6.5 months at 5 years (65 times more than at 1 year). After multiple devices, it reached 14 months, involving on average 1.6 devices (i.e., 8.8 months per device implanted). Moreover, while over a short window (e.g., 2 years), lower-mortality patients may gain less than higher-mortality patients (1.4 vs. 2.3 months), their positions reverse by 15 years (16.0 vs. 13.7 months).
Lifespan gain from biventricular pacing rises nonlinearly with time. Early on, higher-risk patients exhibit more gain, but later, lower-risk patients exhibit more gain. Quantifying gain over less than a patient's lifetime underestimates lifespan gain. Over the first 1 or 2 years, lower-risk patients may seem to gain less, although they may ultimately be the ones who gain the most.
本研究旨在探讨不同计算窗持续时间对预期寿命延长的影响(临床试验中观察到的),以及哪些患者获益最大。
双心室起搏(心脏再同步治疗[CRT])的标志性临床试验通常持续时间不足 1 个设备电池寿命,因此可能会低估在更长时间内的预期寿命获益。
我们对双心室起搏临床试验进行了荟萃分析,以计算预期寿命的延长:首先,在随机对照试验数据的持续时间内,截至 2 年;其次,在典型的 5 年电池寿命内;第三,超过 1 个电池寿命。重要的是,我们应用了戈珀特法来计算与非 CRT 可预防原因相关的死亡率随年龄的增加。
5 项标志性临床试验(COMPANION[心力衰竭的药物治疗、起搏和除颤比较]、CARE-HF[心力衰竭的心脏再同步治疗]、MADIT-CRT[多中心自动除颤器植入试验伴心脏再同步治疗]、REVERSE[再同步逆转收缩性左心室功能障碍的重构]、RAFT[心力衰竭的再同步-除颤])提供了 2 年(6561 例患者)的数据,平均风险比为 0.71。所有试验的预期寿命延长呈非线性增加,从第 1 年的 0.1 个月,到第 2 年的 0.5 个月,预计在第 5 年的 6.5 个月(比第 1 年增加 65 倍)。在多次更换设备后,预期寿命延长可达 14 个月,平均植入 1.6 个设备(即每个植入设备的预期寿命延长 8.8 个月)。此外,虽然在较短的时间窗口(如 2 年)内,低死亡率患者的获益可能小于高死亡率患者(1.4 个月与 2.3 个月),但这种差异会在 15 年内逆转(16.0 个月与 13.7 个月)。
双心室起搏的预期寿命延长呈非线性增加。早期,高风险患者的获益更大,但后期,低风险患者的获益更大。在不到患者寿命的时间内对获益进行量化会低估预期寿命的延长。在最初的 1 到 2 年内,低风险患者可能看起来获益较少,但最终可能是他们获益最多。