Section of Nephrology, Yale University School of Medicine, Veterans Affairs Medical Center, and the Program of Applied Translational Research, New Haven, Connecticut, USA.
PLoS One. 2013 Aug 29;8(8):e71784. doi: 10.1371/journal.pone.0071784. eCollection 2013.
To perform a systematic review of randomized controlled trials to determine whether prevention or slowing of progression of chronic kidney disease would translate into improved mortality, and if so, the attributable risk due to CKD itself on mortality.
CKD is associated with increased mortality. This association is largely based on evidence from the observational studies and evidence from randomized controlled trials is lacking.
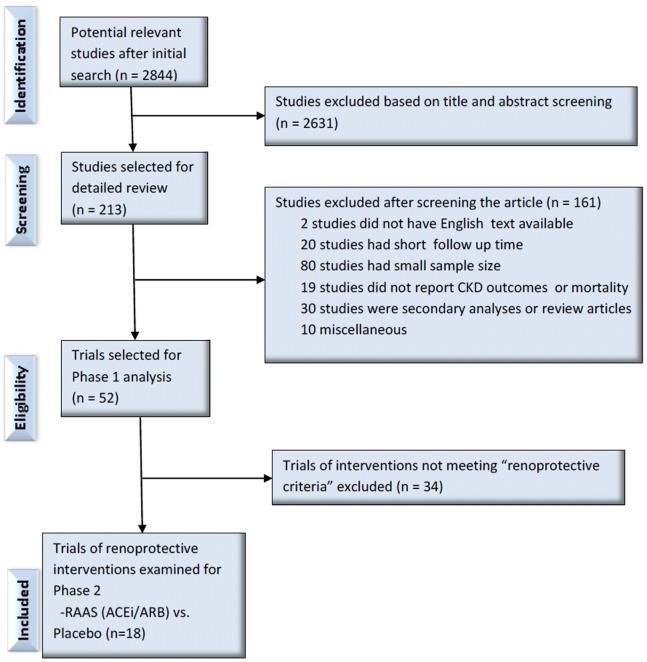
We searched Ovid, Medline and Embase for RCTs in which an intervention was given to prevent or slow the progression of CKD and mortality was reported as primary, secondary or adverse outcomes were eligible and selected. For the first phase, pooled relative risks for renal endpoints were assessed. For the second phase, we assessed the effect on mortality in trials of interventions that definitively reduced CKD endpoints.
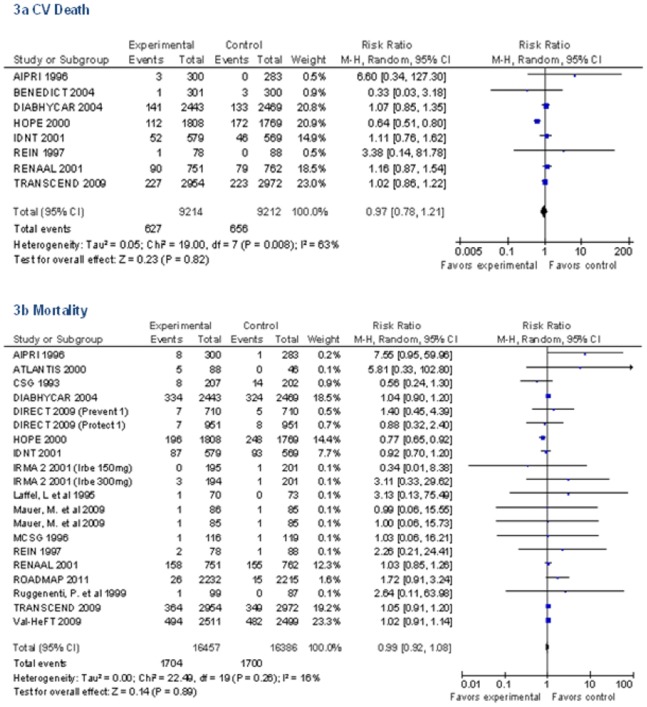
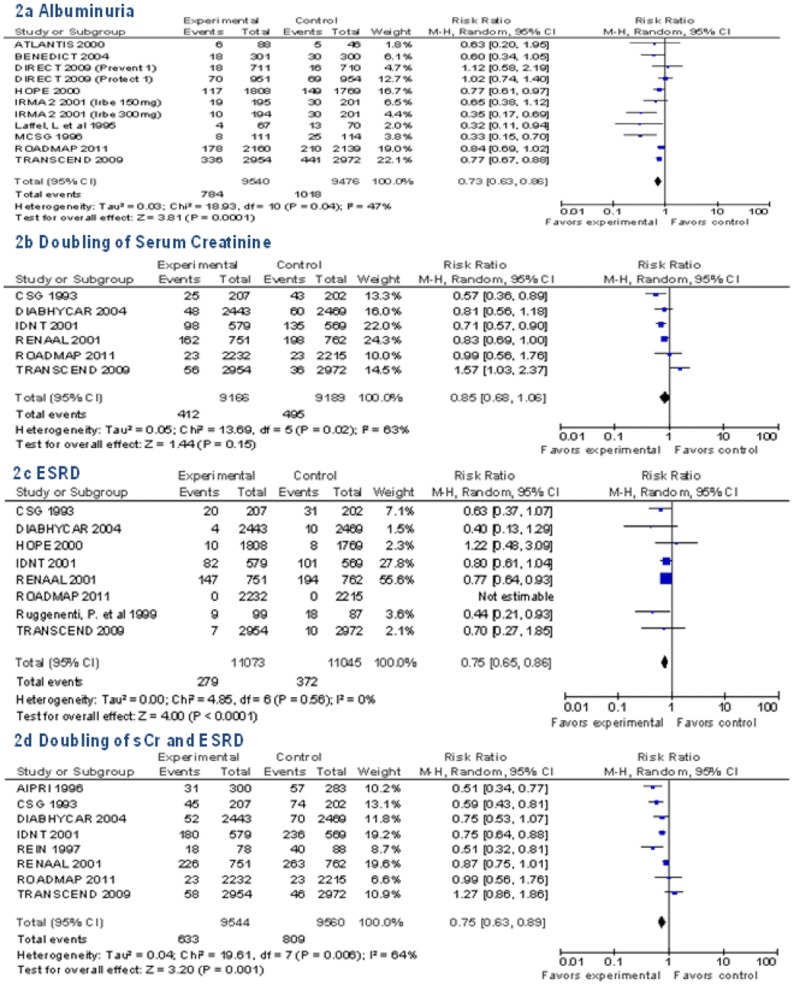
Among 52 studies selected in first phase, only renin-angiotensin-aldosterone-system blockade vs. placebo (n = 18 trials, 32,557 participants) met the efficacy criteria for further analysis in the second phase by reducing renal endpoints 15 to 27% compared to placebo. There was no difference in all-cause mortality (RR 0.99, 95% CI 0.92 to 1.08) or CV death (RR 0.97, 95% CI 0.78 to 1.21) between the treatment and control groups in these trials. There was sufficient statistical power to detect a 9% relative risk reduction in all-cause mortality and a 14% relative risk reduction in cardiovascular mortality.
Firm evidence is lacking that prevention of CKD translates into reductions in mortality. Larger trials with longer follow-up time are needed to determine the benefit of CKD prevention on survival.
系统评价随机对照试验,以确定慢性肾脏病的预防或进展延缓是否会转化为死亡率的改善,以及如果是这样,CKD 本身对死亡率的归因风险。
CKD 与死亡率增加相关。这种关联主要基于观察性研究的证据,缺乏随机对照试验的证据。
我们在 Ovid、Medline 和 Embase 中搜索了 RCTs,其中干预措施用于预防或减缓 CKD 的进展,并且将死亡率作为主要、次要或不良结局进行报告。在第一阶段,评估了肾脏终点的汇总相对风险。在第二阶段,我们评估了在明确降低 CKD 终点的干预试验中对死亡率的影响。
在第一阶段选择的 52 项研究中,只有肾素-血管紧张素-醛固酮系统阻滞剂与安慰剂(n=18 项试验,32557 名参与者)符合进一步分析的疗效标准,与安慰剂相比,肾脏终点降低了 15%至 27%。在这些试验中,治疗组和对照组之间的全因死亡率(RR 0.99,95%CI 0.92 至 1.08)或心血管死亡率(RR 0.97,95%CI 0.78 至 1.21)均无差异。这些试验具有足够的统计学效能来检测全因死亡率降低 9%和心血管死亡率降低 14%的相对风险。
缺乏确凿的证据表明预防 CKD 可降低死亡率。需要进行更大规模、随访时间更长的试验,以确定 CKD 预防对生存的益处。