Chen Yin-Cheng, Weng Shuen-Fu, Hsu Yu-Juei, Wei Chung-Jen, Chiu Chiung-Hsuan
Division of Nephrology, Department of Internal Medicine, Taipei Hospital, Ministry of Health and Welfare, Taipei, Taiwan.
Division of Endocrinology and Metabolism, Department of Internal Medicine, Taipei Medical University Hospital, Taipei, Taiwan.
BMJ Open. 2020 Dec 29;10(12):e041149. doi: 10.1136/bmjopen-2020-041149.
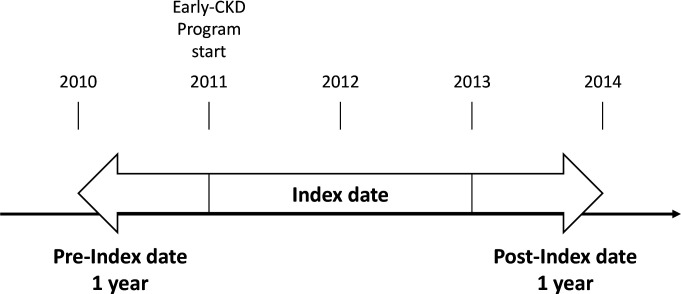
To control and prevent the burdens associated with chronic kidney disease (CKD), Taiwan's National Health Insurance Administration (NHIA) launched the 'early-CKD programme' in 2011 to extend care and education to patients with CKD. This study aims to evaluate the effectiveness of the early-CKD programme in terms of continuity of care (COC).
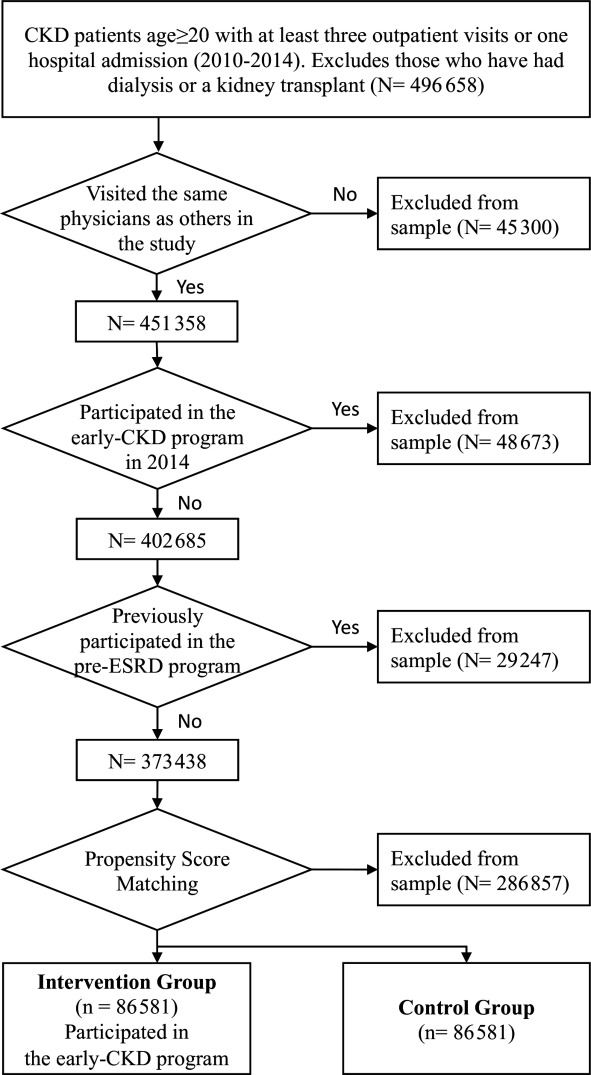
This study used secondary data from 2010 to 2014 provided by the NHIA to identify 86 581 participants each for the intervention and control groups. Patients with CKD who participated in the early-CKD programme between 2011 and 2013 were defined as the intervention group. For the control group, propensity score matching was used to select patients with CKD who did not participate in the programme, but were seen by the same group of physicians.
A multidisciplinary care model for patients with early CKD launched in 2011.
Outcome variables included the continuity of care index (COCI), which measures a physician's COC; number of essential examinations; and resource utilisation. To better identify the difference between groups, we separated COCI into two groups based on mean: high (above mean) and low (below mean). A generalised estimating equation model was used to examine the effects of the early-CKD programme.
The programme significantly increased the number of essential examinations/tests administered to patients (β=0.61, p<0.001) and improved COCI between physicians and patients (OR=4.18, p<0.001). Medical expenses (β=1.03, p<0.001) and medication expenses (β=0.23, p<0.001) significantly increased after the programme was implemented, but patients' kidney-related hospitalisations and emergency department visits decreased (β=-0.13, p<0.001).
From the COC viewpoint, the programme in Taiwan showed a positive effect on COCI, number of essential examinations and resource utilisation.
为控制和预防与慢性肾脏病(CKD)相关的负担,台湾地区国民健康保险署(NHIA)于2011年启动了“早期CKD计划”,以向CKD患者提供护理和教育。本研究旨在评估早期CKD计划在护理连续性(COC)方面的有效性。
本研究使用了NHIA提供的2010年至2014年的二手数据,为干预组和对照组分别确定了86581名参与者。2011年至2013年期间参加早期CKD计划的CKD患者被定义为干预组。对于对照组,采用倾向得分匹配法选择未参加该计划但由同一组医生诊治的CKD患者。
2011年推出的针对早期CKD患者的多学科护理模式。
结局变量包括护理连续性指数(COCI),用于衡量医生的COC;必要检查的次数;以及资源利用情况。为了更好地识别组间差异,我们根据均值将COCI分为两组:高(均值以上)和低(均值以下)。使用广义估计方程模型来检验早期CKD计划的效果。
该计划显著增加了对患者进行的必要检查/测试的次数(β=0.61,p<0.001),并改善了医生与患者之间的COCI(OR=4.18,p<0.001)。该计划实施后,医疗费用(β=1.03,p<0.001)和药物费用(β=0.23,p<0.001)显著增加,但患者与肾脏相关的住院和急诊就诊次数减少(β=-0.13,p<0.001)。
从COC的角度来看,台湾地区的该计划对COCI、必要检查次数和资源利用产生了积极影响。