Matheson Flora I, Smith Katherine L W, Moineddin Rahim, Dunn James R, Glazier Richard H
Centre for Research on Inner City Health at The Keenan Research Centre in the Li Ka Shing Knowledge Institute of St. Michael's Hospital, , Toronto, Ontario, Canada.
J Epidemiol Community Health. 2014 Jan;68(1):64-70. doi: 10.1136/jech-2013-202838. Epub 2013 Sep 6.
There is a growing interest in understanding the connection between mental illness (MI) and the onset of new physical illnesses among previously physically healthy individuals. Yet the role of gender is often forgotten in research focused on comorbidity of health problems. The objective of this study was to examine gender differences in the onset of physical illness in a cohort of respondents who met criteria for MI compared with a control cohort without mental health problems.
This cohort study, conducted in Ontario, Canada, used a unique linked dataset with information from the 2000-2001 Canadian Community Health Survey and medical records (n=15,902). We used adjusted Cox proportional survival analysis to examine risk of onset of four physical health problems (chronic obstructive pulmonary disorder, asthma, hypertension and diabetes) for those with and without baseline MI across a 10-year period (2002-2011) among respondents aged 18-74 years. We controlled for socioeconomic and health indicators associated with health.
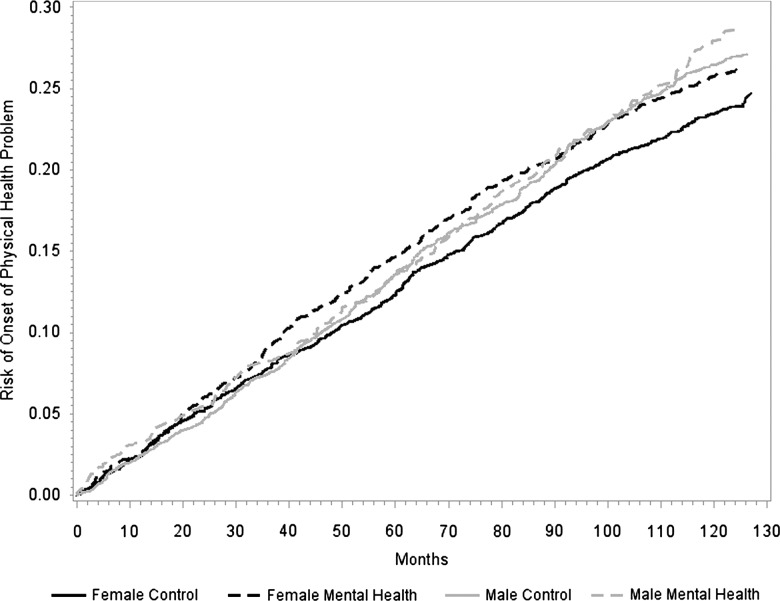
The incidence of physical illness in the MI cohort was 28.5% among women and 29.9% among men (p=0.85) relative to controls (23.8% and 24%, respectively; p=0.48). Women in the MI cohort developed secondary physical health problems a year earlier than their male counterparts (p=0.002). Findings from the Cox proportional survival regression showed that women were at 14% reduced risk of developing physical illness, meaning that men were more disadvantaged (HR=0.89, CI 0.80 to 0.98). Those in the MI cohort were at 10 times greater risk of developing a secondary physical illness over the 10-year period (HR=1.10, CI 0.98 to 1.21). There was no significant interaction between gender and MI cohort (HR=1.05, CI 0.85 to 1.27).
Policy and clinical practice have to be sensitive to these complex-needs patients. Gender-specific treatment and prevention practices can be developed to target those at higher risk of multiple health conditions.
对于理解精神疾病(MI)与既往身体健康个体中新发躯体疾病发作之间的联系,人们的兴趣日益浓厚。然而,在关注健康问题共病的研究中,性别因素常常被忽视。本研究的目的是在一组符合MI标准的受访者队列中,与无心理健康问题的对照队列相比,研究躯体疾病发作中的性别差异。
这项队列研究在加拿大安大略省进行,使用了一个独特的关联数据集,其中包含2000 - 2001年加拿大社区健康调查和医疗记录的信息(n = 15,902)。我们使用调整后的Cox比例生存分析,来研究18 - 74岁受访者中,有和无基线MI的人群在10年期间(2002 - 2011年)出现四种躯体健康问题(慢性阻塞性肺疾病、哮喘、高血压和糖尿病)的风险。我们对与健康相关的社会经济和健康指标进行了控制。
相对于对照组(女性分别为23.8%,男性为24%;p = 0.48),MI队列中女性的躯体疾病发病率为28.5%,男性为29.9%(p = 0.85)。MI队列中的女性比男性早一年出现继发性躯体健康问题(p = 0.002)。Cox比例生存回归的结果显示,女性出现躯体疾病的风险降低了14%,这意味着男性处于更不利的地位(风险比[HR]=0.89,95%置信区间[CI]为0.80至0.98)。在10年期间,MI队列中的人群出现继发性躯体疾病的风险高出10倍(HR = 1.10,CI为0.98至1.21)。性别与MI队列之间没有显著的交互作用(HR = 1.05,CI为0.85至1.27)。
政策和临床实践必须对这些有复杂需求的患者保持敏感。可以制定针对性别的治疗和预防措施,以针对那些有多种健康状况高风险人群。