Service de réanimation médicale, Hôpital Saint-Antoine, Assistance Publique-Hôpitaux de Paris, 184 rue du Faubourg Saint-Antoine, Cedex 12, Paris 75571, France.
Ann Intensive Care. 2013 Sep 16;3(1):31. doi: 10.1186/2110-5820-3-31.
Mottling score has been reported to be a strong predictive factor during septic shock. However, the pathophysiology of mottling remains unclear.
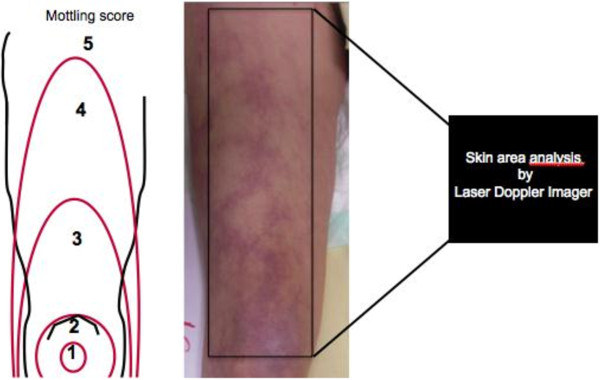
In patients admitted in ICU for septic shock, we measured on the same area the mean skin perfusion by laser Doppler, the mottling score, and variations of both indices between T1 (6 hours after vasopressors were started) and T2 (24 hours later).
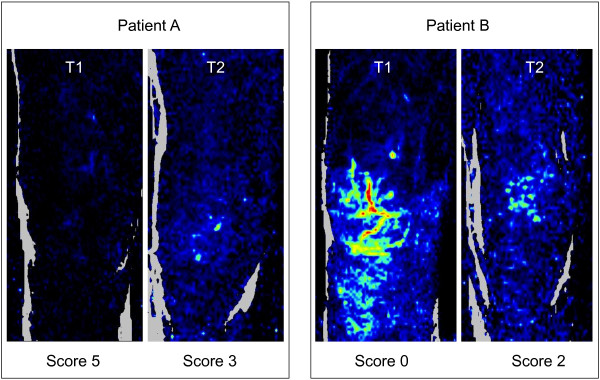
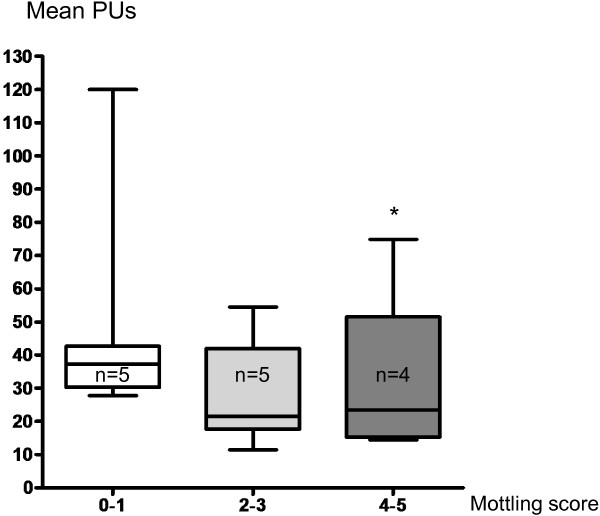
Fourteen patients were included, SAPS II was 56 [37-71] and SOFA score at T1 was 10 [7-12]. The mean skin surface area analyzed was 4108 ± 740 mm2; 1184 ± 141 measurements were performed over each defined skin surface area. Skin perfusion was significantly different according to mottling score and decreased from 37 [31-42] perfusion units (PUs) for a mottling score of [0-1] to 22 [20-32] PUs for a mottling score of [2-3] and 23 [16-28] for a score of [4-5] (Kruskal-Wallis test, P = 0.05). We analyzed skin perfusion changes during resuscitation in each patient and together with mottling score variations between T1 and T2 using a Wilcoxon signed-rank test. Among the 14 patients included, mottling score increased (worsened) in 5 patients, decreased (improved) in 5 patients, and remained stable in 4 patients. Baseline skin perfusion at T1 was arbitrarily scored 100%. Mean skin perfusion significantly decreased in all the patients whose mottling score worsened from 100% baseline to 63.2 ± 10.7% (P = 0.001), mean skin perfusion significantly increased in all patients whose mottling score improved from 100% baseline to 172.6 ± 46.8% (P = 0.001), and remained stable in patients whose mottling score did not change (100.5 ± 6.8%, P = 0.95).
We have shown that mottling score variations and skin perfusion changes during septic shock resuscitation were correlated, providing additional evidence that mottling reflects skin hypoperfusion.
斑驳评分已被报道为感染性休克期间的一个强有力的预测因素。然而,斑驳的病理生理学仍然不清楚。
在因感染性休克而入住 ICU 的患者中,我们在同一区域测量激光多普勒的平均皮肤灌注,斑驳评分,以及 T1(开始使用加压素后 6 小时)和 T2(24 小时后)之间两个指数的变化。
共纳入 14 例患者,SAPS II 为 56 [37-71],T1 时 SOFA 评分为 10 [7-12]。分析的平均皮肤表面积为 4108 ± 740 mm2;在每个定义的皮肤表面上进行了 1184 ± 141 次测量。皮肤灌注根据斑驳评分而显著不同,从斑驳评分为[0-1]的 37 [31-42]灌注单位(PU)下降到斑驳评分为[2-3]的 22 [20-32] PU,以及评分[4-5]的 23 [16-28] PU(Kruskal-Wallis 检验,P = 0.05)。我们分析了每个患者复苏过程中的皮肤灌注变化,并使用 Wilcoxon 符号秩检验分析了 T1 和 T2 之间斑驳评分的变化。在纳入的 14 例患者中,5 例患者的斑驳评分增加(恶化),5 例患者的斑驳评分减少(改善),4 例患者的斑驳评分稳定。T1 时的基线皮肤灌注任意评分为 100%。所有斑驳评分恶化的患者的平均皮肤灌注显著下降,从基线的 100%降至 63.2 ± 10.7%(P = 0.001),所有斑驳评分改善的患者的平均皮肤灌注显著增加,从基线的 100%增加到 172.6 ± 46.8%(P = 0.001),而斑驳评分不变的患者则保持稳定(100.5 ± 6.8%,P = 0.95)。
我们已经表明,感染性休克复苏期间斑驳评分的变化和皮肤灌注的变化是相关的,这提供了额外的证据表明斑驳反映了皮肤低灌注。