James Buchanan Brady Urological Institute, Johns Hopkins Medical Institutions, Baltimore, Maryland.
James Buchanan Brady Urological Institute, Johns Hopkins Medical Institutions, Baltimore, Maryland.
J Urol. 2014 Mar;191(3):629-37. doi: 10.1016/j.juro.2013.09.029. Epub 2013 Sep 20.
Prostate specific antigen velocity is an unreliable predictor of adverse pathology findings in patients on active surveillance for low risk prostate cancer. However, to our knowledge a new concept called prostate specific antigen velocity risk count, recently validated in a screening cohort, has not been investigated in an active surveillance cohort.
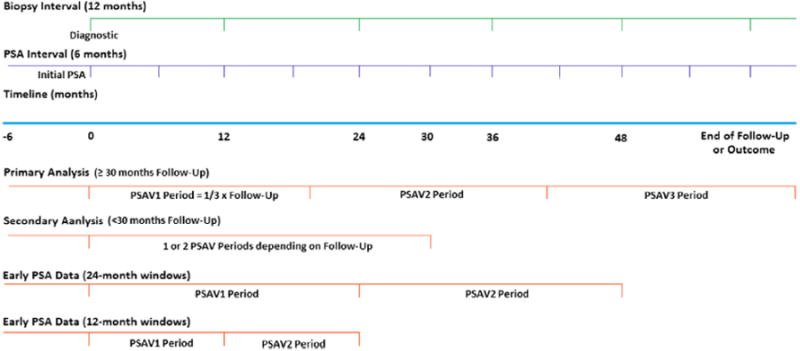
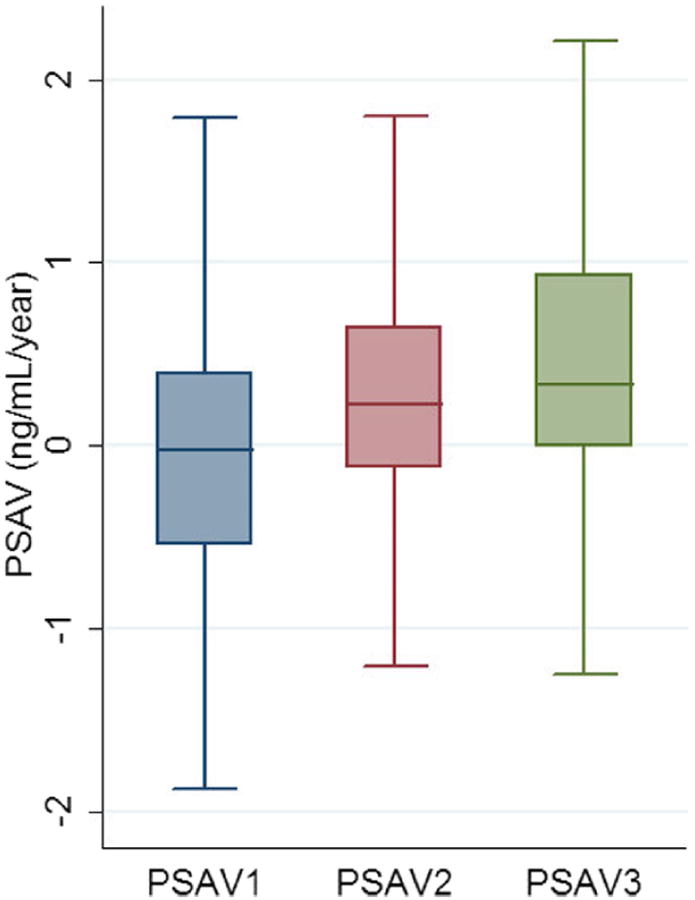
We evaluated a cohort of men from 1995 to 2012 with prostate cancer on active surveillance. They had stage T1c disease, prostate specific antigen density less than 0.15 ng/ml, Gleason score 6 or less, 2 or fewer biopsy cores and 50% or less involvement of any core with cancer. The men were observed by semiannual prostate specific antigen measurements, digital rectal examinations and an annual surveillance biopsy. Treatment was recommended for biopsy reclassification. Patients with 30 months or greater of followup and 3 serial prostate specific antigen velocity measurements were used in primary analysis by logistic regression, Cox proportional hazards, Kaplan-Meier analysis and performance parameters, including the AUC of the ROC curve.
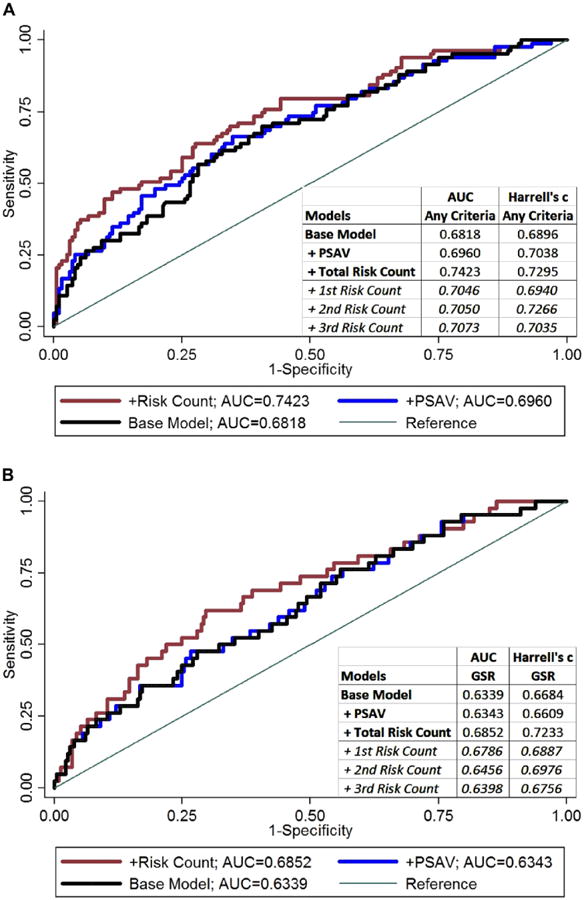
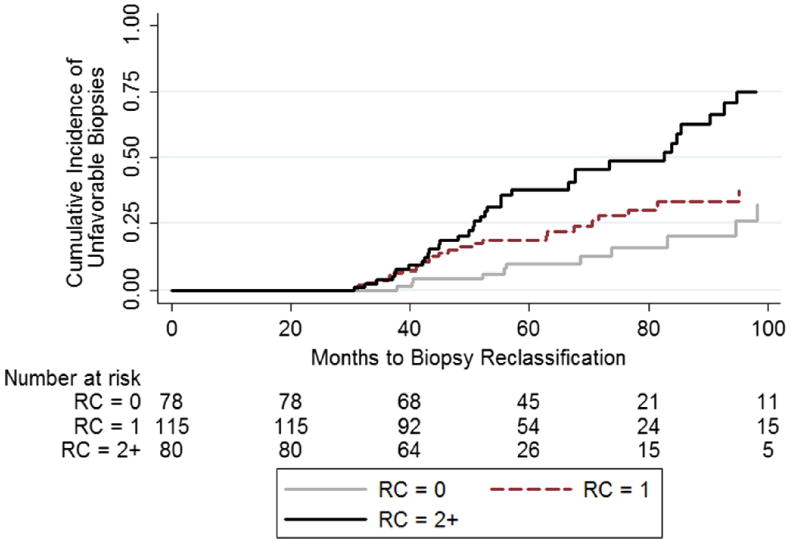
Primary analysis included 275 of 668 men who met very low risk inclusion criteria, of whom 83 (30.2%) were reclassified at a median of 57.1 months. Reclassification risk increased with risk count, that is a risk count of 3 (HR 4.63, 95% CI 1.54-13.87) and 2 (HR 3.73, 95% CI 1.75-7.97) compared to zero. Results were similar for Gleason score reclassification (HR 7.45, 95% CI 1.60-34.71 and 3.96, 95% CI 1.35-11.62, respectively). On secondary analysis the negative predictive value (risk count 1 or less) was 91.5% for reclassification in the next year. Adding the prostate specific antigen velocity risk count improved the AUC in a model including baseline prostate specific antigen density (0.7423 vs 0.6818, p = 0.025) and it outperformed the addition of overall prostate specific antigen velocity (0.7423 vs 0.6960, p = 0.037).
Prostate specific antigen velocity risk count may be useful for monitoring patients on active surveillance and decreasing the frequency of biopsies needed in the long term.
前列腺特异性抗原速度是预测低危前列腺癌主动监测患者不良病理发现的不可靠指标。然而,据我们所知,最近在筛查队列中验证的一个新概念,即前列腺特异性抗原速度风险计数,尚未在主动监测队列中进行研究。
我们评估了 1995 年至 2012 年间在主动监测中患有前列腺癌的男性队列。他们患有 T1c 期疾病,前列腺特异性抗原密度小于 0.15ng/ml,Gleason 评分为 6 分或更低,活检核心数为 2 个或更少,且任何核心中癌症的受累比例为 50%或更少。通过半年度前列腺特异性抗原测量、数字直肠检查和年度监测活检对男性进行观察。建议对活检重新分类进行治疗。在主要分析中,我们使用逻辑回归、Cox 比例风险、Kaplan-Meier 分析和性能参数,包括 ROC 曲线的 AUC,对具有 30 个月或更长时间随访和 3 次连续前列腺特异性抗原速度测量的 275 名符合极低风险纳入标准的患者进行了初步分析。重新分类风险随着风险计数的增加而增加,即与零相比,风险计数为 3(HR 4.63,95%CI 1.54-13.87)和 2(HR 3.73,95%CI 1.75-7.97)。Gleason 评分重新分类的结果也相似(HR 分别为 7.45,95%CI 1.60-34.71 和 3.96,95%CI 1.35-11.62)。在二次分析中,下一年重新分类的阴性预测值(风险计数为 1 或更少)为 91.5%。在包括基线前列腺特异性抗原密度的模型中添加前列腺特异性抗原速度风险计数(0.7423 对 0.6818,p=0.025),并优于添加总体前列腺特异性抗原速度(0.7423 对 0.6960,p=0.037)。
前列腺特异性抗原速度风险计数可用于监测主动监测患者,并减少长期所需的活检频率。