1] Department of Neuroradiology, Aarhus University Hospital, Aarhus, Denmark [2] Center of Functionally Integrative Neuroscience and MINDLab, Aarhus University, Aarhus, Denmark.
J Cereb Blood Flow Metab. 2013 Dec;33(12):1825-37. doi: 10.1038/jcbfm.2013.173. Epub 2013 Sep 25.
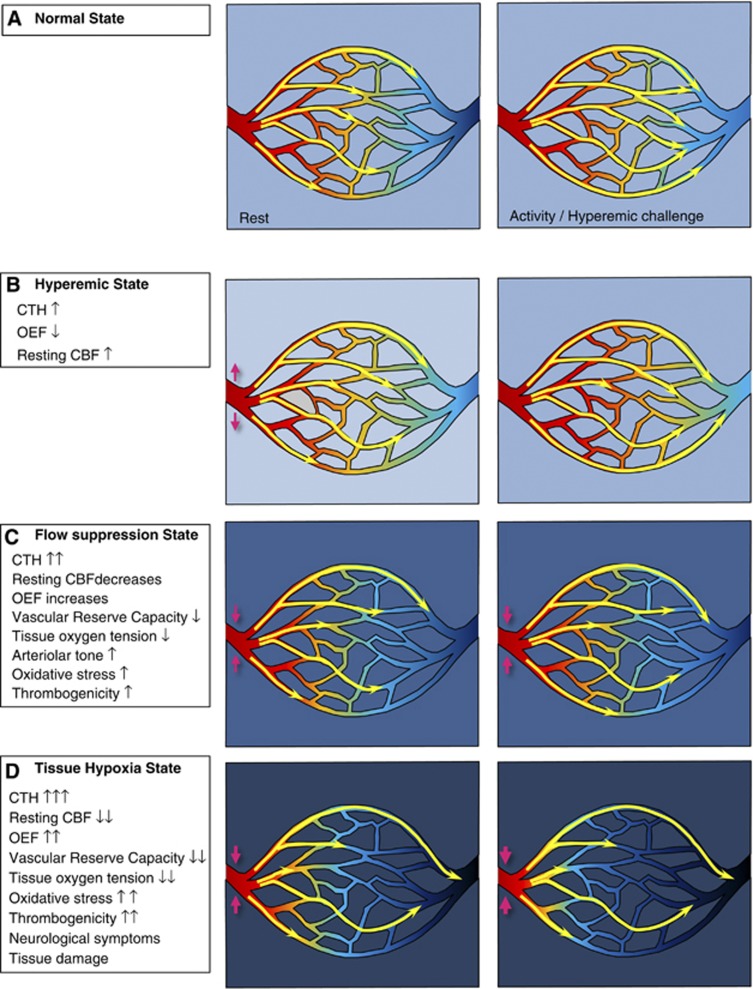
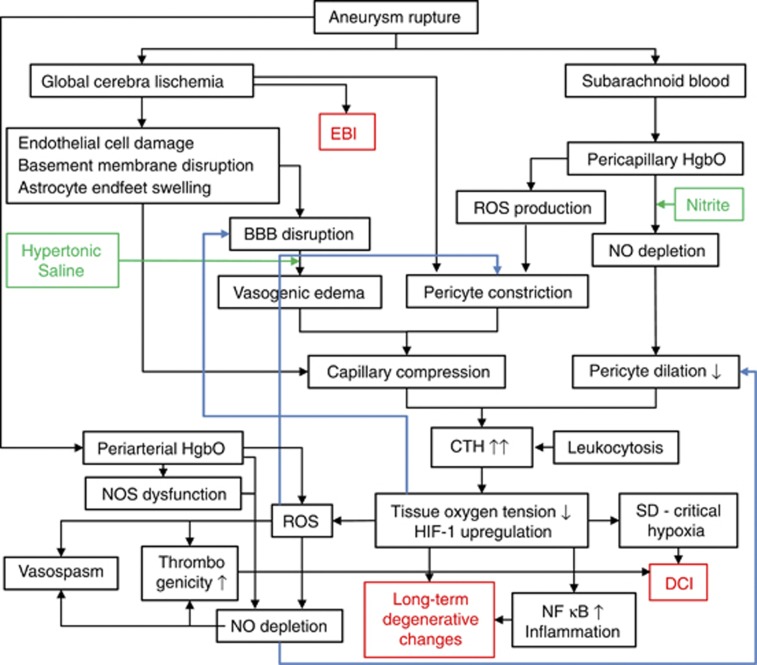
The mortality after aneurysmal subarachnoid hemorrhage (SAH) is 50%, and most survivors suffer severe functional and cognitive deficits. Half of SAH patients deteriorate 5 to 14 days after the initial bleeding, so-called delayed cerebral ischemia (DCI). Although often attributed to vasospasms, DCI may develop in the absence of angiographic vasospasms, and therapeutic reversal of angiographic vasospasms fails to improve patient outcome. The etiology of chronic neurodegenerative changes after SAH remains poorly understood. Brain oxygenation depends on both cerebral blood flow (CBF) and its microscopic distribution, the so-called capillary transit time heterogeneity (CTH). In theory, increased CTH can therefore lead to tissue hypoxia in the absence of severe CBF reductions, whereas reductions in CBF, paradoxically, improve brain oxygenation if CTH is critically elevated. We review potential sources of elevated CTH after SAH. Pericyte constrictions in relation to the initial ischemic episode and subsequent oxidative stress, nitric oxide depletion during the pericapillary clearance of oxyhemoglobin, vasogenic edema, leukocytosis, and astrocytic endfeet swelling are identified as potential sources of elevated CTH, and hence of metabolic derangement, after SAH. Irreversible changes in capillary morphology and function are predicted to contribute to long-term relative tissue hypoxia, inflammation, and neurodegeneration. We discuss diagnostic and therapeutic implications of these predictions.
蛛网膜下腔出血(SAH)后的死亡率为 50%,大多数幸存者都有严重的功能和认知障碍。大约一半的 SAH 患者在初始出血后 5 至 14 天病情恶化,即所谓的迟发性脑缺血(DCI)。尽管 DCI 通常归因于血管痉挛,但在没有血管造影血管痉挛的情况下也可能发生,并且血管造影血管痉挛的治疗逆转未能改善患者的预后。SAH 后慢性神经退行性改变的病因仍知之甚少。脑氧合既取决于脑血流量(CBF),也取决于其微观分布,即所谓的毛细血管渡越时间异质性(CTH)。因此,理论上,即使 CBF 严重减少,增加 CTH 也可能导致组织缺氧,而 CBF 减少,如果 CTH 严重升高,则会改善脑氧合。我们回顾了 SAH 后 CTH 升高的潜在来源。与初始缺血事件和随后的氧化应激有关的周细胞收缩、氧合血红蛋白在毛细血管清除过程中的一氧化氮耗竭、血管源性水肿、白细胞增多和星形胶质细胞终足肿胀被认为是 CTH 升高的潜在来源,因此也是代谢紊乱的潜在来源SAH 后。毛细血管形态和功能的不可逆变化预计会导致长期相对组织缺氧、炎症和神经退行性变。我们讨论了这些预测的诊断和治疗意义。