Stephens Jennifer M, Gao Xin, Patel Dipen A, Verheggen Bram G, Shelbaya Ahmed, Haider Seema
Pharmerit North America, Bethesda, MD, USA.
Clinicoecon Outcomes Res. 2013 Sep 16;5:447-57. doi: 10.2147/CEOR.S46991. eCollection 2013.
Previous economic analyses evaluating treatment of methicillin-resistant Staphylococcus aureus (MRSA) complicated skin and soft-tissue infections (cSSTI) failed to include all direct treatment costs such as outpatient parenteral antibiotic therapy (OPAT). Our objective was to develop an economic model from a US payer perspective that includes all direct inpatient and outpatient costs incurred by patients with MRSA cSSTI receiving linezolid, vancomycin, or daptomycin.
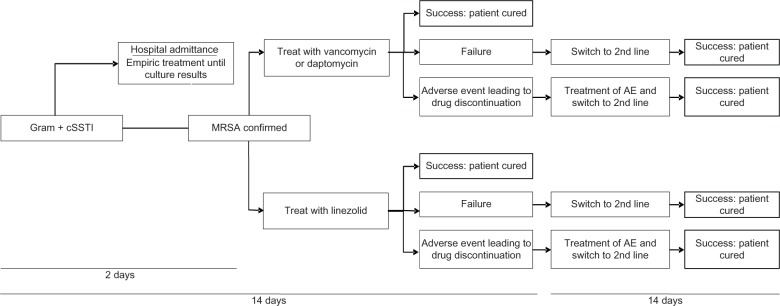
A 4-week decision model was developed for this economic analysis. Published literature and database analyses with validation by experts provided clinical, resource use, and cost inputs on data such as efficacy rate, length of stay, adverse events, and OPAT services. Base-case analysis assumed equal efficacy and equal length of stay for treatments. We conducted several sensitivity analyses where assumptions on resource use or efficacy were varied. Costs were reported in year-end 2011 US dollars.
Total treatment costs in the base-case were lower for linezolid ($10,571) than vancomycin ($11,096), and daptomycin ($13,612). Inpatient treatment costs were $740 more, but outpatient costs, $1,266 less with linezolid than vancomycin therapy due to a switch to oral linezolid when the patient was discharged. Compared with daptomycin, both inpatient and outpatient treatment costs were lower with linezolid by $87 and $2,954 respectively. In sensitivity analyses, linezolid had lower costs compared with vancomycin and daptomycin when using differential length of stay data from a clinical trial, and using success rates from a meta-analysis. In a scenario without peripherally inserted central catheter line costs, linezolid became slightly more expensive than vancomycin (by $285), but remained less costly than daptomycin (by $2,316).
Outpatient costs of managing MRSA cSSTI may be reduced by 30%-50% with oral linezolid compared with vancomycin or daptomycin. Results from this analysis support potential economic benefit and cost savings of using linezolid versus traditional OPAT when total inpatient and outpatient medical costs are evaluated.
以往评估耐甲氧西林金黄色葡萄球菌(MRSA)复杂皮肤和软组织感染(cSSTI)治疗的经济分析未纳入所有直接治疗成本,如门诊胃肠外抗生素治疗(OPAT)。我们的目标是从美国医保支付方的角度建立一个经济模型,该模型涵盖接受利奈唑胺、万古霉素或达托霉素治疗的MRSA cSSTI患者产生的所有直接住院和门诊费用。
为该经济分析建立了一个为期4周的决策模型。已发表的文献和数据库分析经专家验证,提供了有关疗效率、住院时间、不良事件和OPAT服务等数据的临床、资源使用和成本投入。基础病例分析假设各治疗方法疗效相同、住院时间相同。我们进行了多项敏感性分析,改变了资源使用或疗效的假设。成本以2011年年末美元报告。
基础病例中,利奈唑胺的总治疗成本(10,571美元)低于万古霉素(11,096美元)和达托霉素(13,612美元)。与万古霉素治疗相比,利奈唑胺的住院治疗成本高740美元,但门诊成本低1,266美元,这是因为患者出院时改用口服利奈唑胺。与达托霉素相比,利奈唑胺的住院和门诊治疗成本分别低87美元和2,954美元。在敏感性分析中,当使用来自一项临床试验的不同住院时间数据以及一项荟萃分析的成功率时,利奈唑胺的成本低于万古霉素和达托霉素。在不考虑外周静脉穿刺中心静脉导管费用的情况下,利奈唑胺的成本比万古霉素略高(285美元),但仍低于达托霉素(2,316美元)。
与万古霉素或达托霉素相比,口服利奈唑胺可使MRSA cSSTI患者的门诊治疗成本降低30% - 50%。当评估住院和门诊医疗总成本时,该分析结果支持使用利奈唑胺相对于传统OPAT具有潜在的经济效益和成本节约。