Vascular Surgery Research Laboratory, Division of Vascular and Endovascular Surgery, Brigham and Women's Hospital, and Harvard Medical School, Boston, MA 02115, USA.
Biochem Pharmacol. 2013 Dec 15;86(12):1627-42. doi: 10.1016/j.bcp.2013.09.024. Epub 2013 Oct 4.
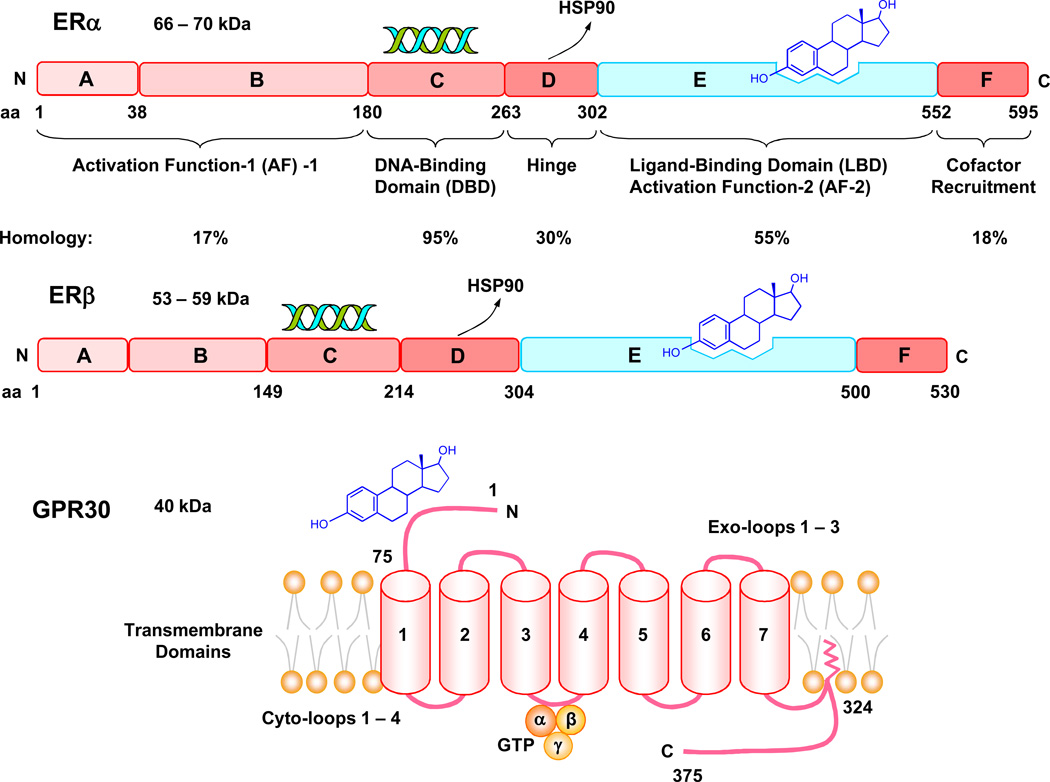
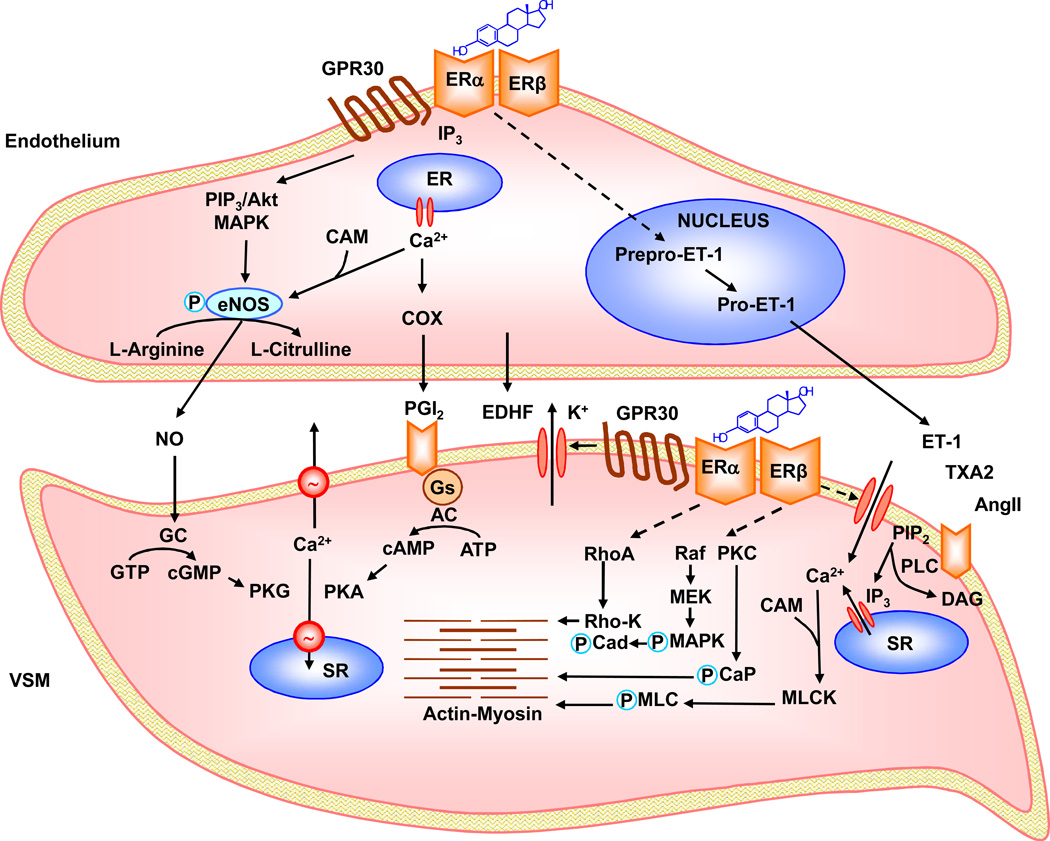
Cardiovascular disease (CVD) is less common in premenopausal women than men of the same age or postmenopausal women, suggesting vascular benefits of estrogen. Estrogen activates estrogen receptors ERα, ERβ and GPR30 in endothelium and vascular smooth muscle (VSM), which trigger downstream signaling pathways and lead to genomic and non-genomic vascular effects such as vasodilation, decreased VSM contraction and growth and reduced vascular remodeling. However, randomized clinical trials (RCTs), such as the Women's Health Initiative (WHI) and Heart and Estrogen/progestin Replacement Study (HERS), have shown little vascular benefits and even adverse events with menopausal hormone therapy (MHT), likely due to factors related to the MHT used, ER profile, and RCT design. Some MHT forms, dose, combinations or route of administration may have inadequate vascular effects. Age-related changes in ER amount, distribution, integrity and post-ER signaling could alter the vascular response to MHT. The subject's age, preexisting CVD, and hormone environment could also reduce the effects of MHT. Further evaluation of natural and synthetic estrogens, phytoestrogens, and selective estrogen-receptor modulators (SERMs), and the design of appropriate MHT combinations, dose, route and 'timing' could improve the effectiveness of conventional MHT and provide alternative therapies in the peri-menopausal period. Targeting ER using specific ER agonists, localized MHT delivery, and activation of specific post-ER signaling pathways could counter age-related changes in ER. Examination of the hormone environment and conditions associated with hormone imbalance such as polycystic ovary syndrome may reveal the causes of abnormal hormone-receptor interactions. Consideration of these factors in new RCTs such as the Kronos Early Estrogen Prevention Study (KEEPS) could enhance the vascular benefits of estrogen in postmenopausal CVD.
心血管疾病(CVD)在绝经前女性中比同年龄男性或绝经后女性少见,提示雌激素对血管有保护作用。雌激素在血管内皮和平滑肌中激活雌激素受体 ERα、ERβ 和 GPR30,触发下游信号通路,导致基因组和非基因组血管效应,如血管扩张、血管平滑肌收缩和生长减少以及血管重塑减少。然而,随机临床试验(RCT),如妇女健康倡议(WHI)和心脏和雌激素/孕激素替代研究(HERS),表明绝经激素治疗(MHT)对血管几乎没有益处,甚至有不良事件,这可能与所用 MHT 相关的因素、ER 谱和 RCT 设计有关。一些 MHT 形式、剂量、组合或给药途径可能对血管的作用不足。ER 数量、分布、完整性和 ER 后信号的年龄相关变化可能改变对 MHT 的血管反应。受试者的年龄、预先存在的 CVD 和激素环境也可能降低 MHT 的效果。进一步评估天然和合成雌激素、植物雌激素和选择性雌激素受体调节剂(SERMs),以及设计适当的 MHT 组合、剂量、途径和“时机”,可以提高传统 MHT 的有效性,并为围绝经期提供替代疗法。使用特定的 ER 激动剂靶向 ER、局部 MHT 给药以及激活特定的 ER 后信号通路,可以对抗 ER 随年龄的变化。检查与激素失衡相关的激素环境和条件,如多囊卵巢综合征,可能揭示异常激素-受体相互作用的原因。在新的 RCT 中考虑这些因素,如 Kronos 早期雌激素预防研究(KEEPS),可以增强绝经后 CVD 中雌激素的血管益处。