Leelarathna Lalantha, Little Stuart A, Walkinshaw Emma, Tan Horng Kai, Lubina-Solomon Alexandra, Kumareswaran Kavita, Lane Annette P, Chadwick Thomas, Marshall Sally M, Speight Jane, Flanagan Daniel, Heller Simon R, Shaw James A M, Evans Mark L
Corresponding author: Mark L. Evans,
Diabetes Care. 2013 Dec;36(12):4063-70. doi: 10.2337/dc13-1004. Epub 2013 Oct 15.
Impaired awareness of hypoglycemia (IAH) and defective counterregulation significantly increase severe hypoglycemia risk in type 1 diabetes (T1D). We evaluated restoration of IAH/defective counterregulation by a treatment strategy targeted at hypoglycemia avoidance in adults with T1D with IAH (Gold score ≥4) participating in the U.K.-based multicenter HypoCOMPaSS randomized controlled trial.
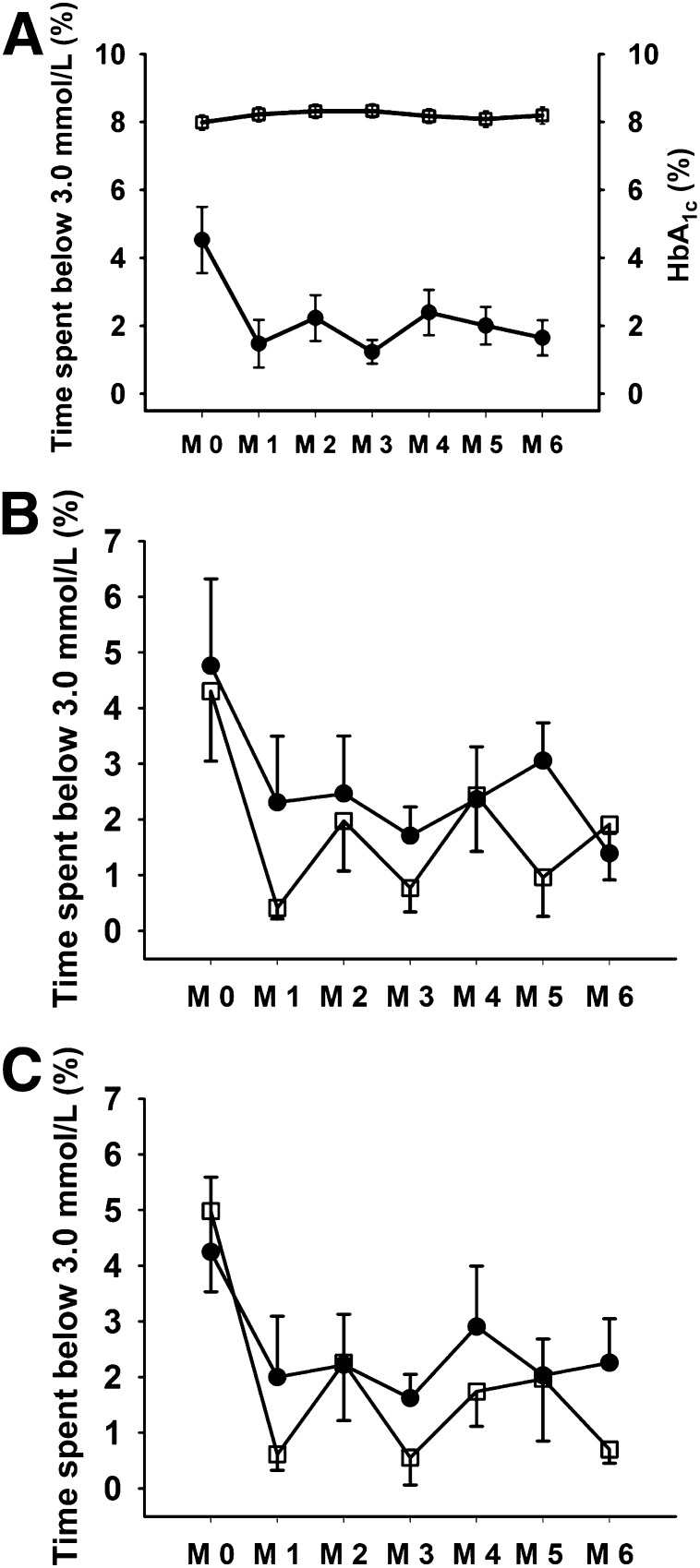
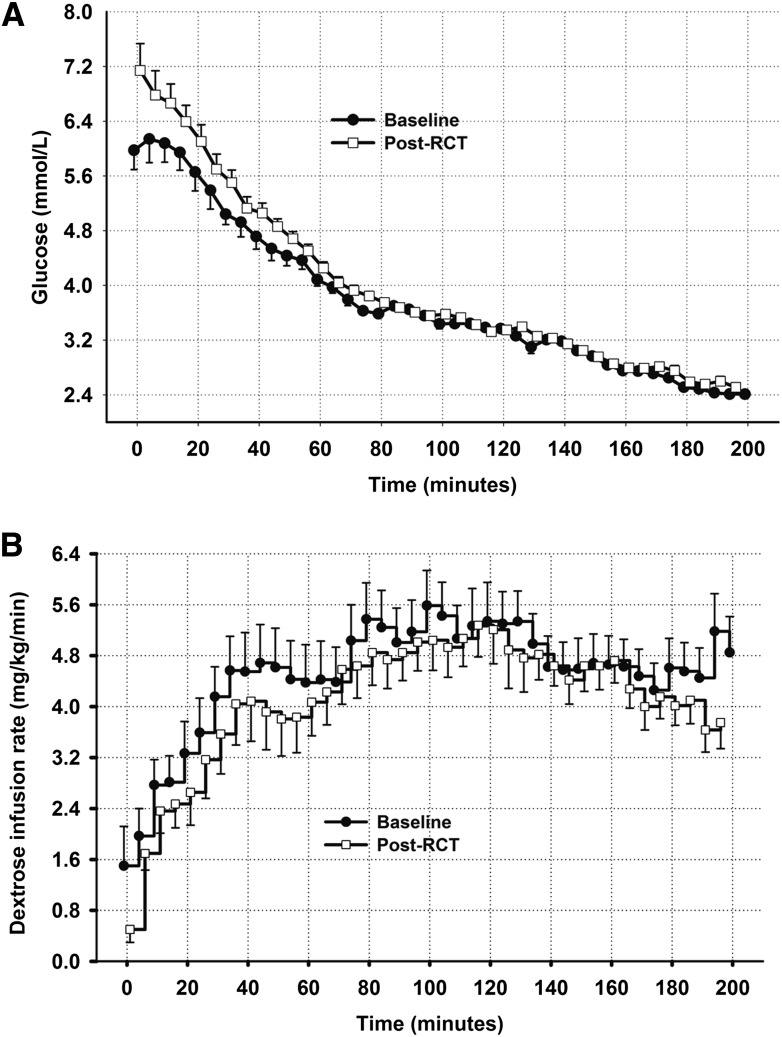
Eighteen subjects with T1D and IAH (mean ± SD age 50 ± 9 years, T1D duration 35 ± 10 years, HbA1c 8.1 ± 1.0% [65 ± 10.9 mmol/mol]) underwent stepped hyperinsulinemic-hypoglycemic clamp studies before and after a 6-month intervention. The intervention comprised the HypoCOMPaSS education tool in all and randomized allocation, in a 2 × 2 factorial study design, to multiple daily insulin analog injections or continuous subcutaneous insulin infusion therapy and conventional glucose monitoring or real-time continuous glucose monitoring. Symptoms, cognitive function, and counterregulatory hormones were measured at each glucose plateau (5.0, 3.8, 3.4, 2.8, and 2.4 mmol/L), with each step lasting 40 min with subjects kept blinded to their actual glucose value throughout clamp studies.
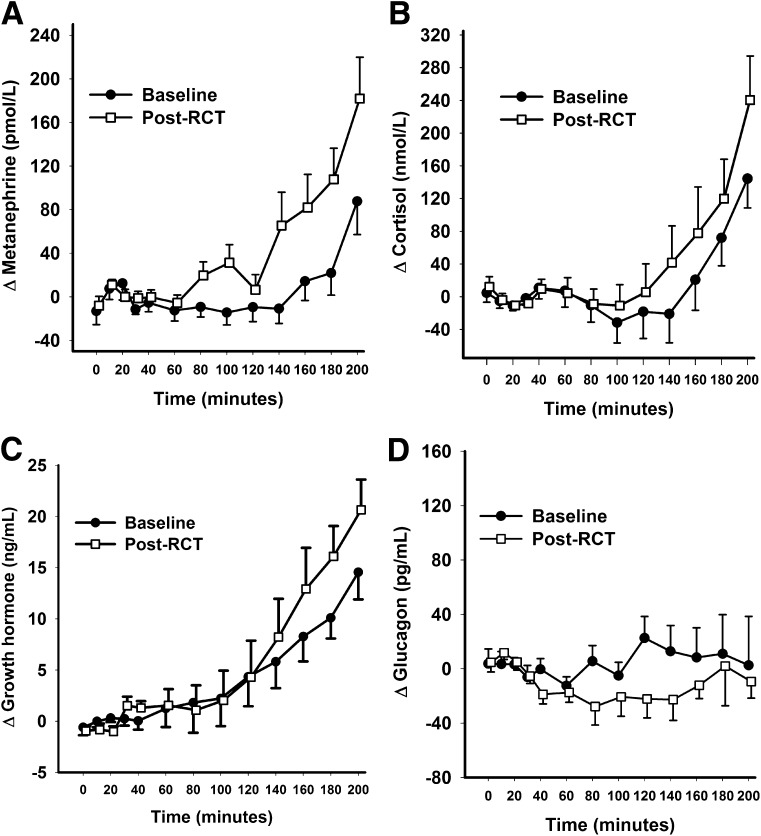
After intervention, glucose concentrations at which subjects first felt hypoglycemic increased (mean ± SE from 2.6 ± 0.1 to 3.1 ± 0.2 mmol/L, P = 0.02), and symptom and plasma metanephrine responses to hypoglycemia were higher (median area under curve for symptoms, 580 [interquartile range {IQR} 420-780] vs. 710 [460-1,260], P = 0.02; metanephrine, 2,412 [-3,026 to 7,279] vs. 5,180 [-771 to 11,513], P = 0.01). Glycemic threshold for deterioration of cognitive function measured by four-choice reaction time was unchanged, while the color-word Stroop test showed a degree of adaptation.
Even in long-standing T1D, IAH and defective counterregulation may be improved by a clinical strategy aimed at hypoglycemia avoidance.
低血糖意识受损(IAH)和反调节功能缺陷会显著增加1型糖尿病(T1D)患者发生严重低血糖的风险。我们在一项基于英国的多中心HypoCOMPaSS随机对照试验中,评估了一种旨在避免低血糖的治疗策略对患有IAH(Gold评分≥4)的成年T1D患者IAH/反调节功能缺陷的恢复情况。
18名患有T1D和IAH的受试者(平均±标准差年龄50±9岁,T1D病程35±10年,糖化血红蛋白8.1±1.0%[65±10.9 mmol/mol])在6个月干预前后进行了逐步高胰岛素-低血糖钳夹研究。干预措施包括全体使用HypoCOMPaSS教育工具,并在2×2析因研究设计中随机分配,接受每日多次胰岛素类似物注射或持续皮下胰岛素输注治疗,以及传统血糖监测或实时连续血糖监测。在每个血糖平台(5.0、3.8、3.4、2.8和2.4 mmol/L)测量症状、认知功能和反调节激素,每个阶段持续40分钟,在整个钳夹研究过程中受试者对其实际血糖值保持盲态。
干预后,受试者首次感觉到低血糖时的血糖浓度升高(平均±标准误从2.6±0.1 mmol/L升至3.1±0.2 mmol/L,P = 0.02),对低血糖的症状和血浆间甲肾上腺素反应增强(症状的曲线下面积中位数,580[四分位间距{IQR}420 - 780]对710[460 - 1260],P = 0.02;间甲肾上腺素,2412[-3026至7279]对5180[-771至11513],P = 0.01)。通过四选反应时间测量的认知功能恶化的血糖阈值未改变,而色词Stroop测试显示出一定程度的适应性。
即使在病程较长的T1D患者中,旨在避免低血糖的临床策略也可能改善IAH和反调节功能缺陷。