Argoti Pedro S, Bebbington Michael, Adler Michael, Johnson Anthony, Moise Kenneth J
Division of Maternal-Fetal Medicine, Department of Obstetrics, Gynecology and Reproductive Medicine, University of Texas School of Medicine at Houston, The Texas Fetal Center, Children's Memorial Hermann Hospital, Houston, Texas.
AJP Rep. 2013 Oct;3(2):75-8. doi: 10.1055/s-0033-1341576. Epub 2013 Mar 19.
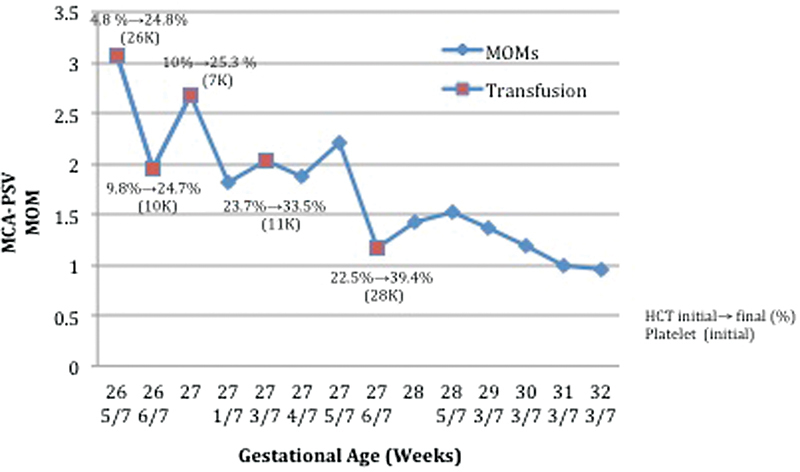
Introduction Fetal exsanguination is a rare complication of cordocentesis. Successful correction of fetal thrombocytopenia is essential for the reduction of risks. Case Report A 25-year-old, gravida 3, P2-0-0-0-2, was referred at 27 weeks of gestation for evaluation of newly diagnosed nonimmune hydrops secondary to parvovirus infection. Despite the use of ancillary platelet transfusions to correct the severe fetal thrombocytopenia, prolonged bleeding from the cord puncture site still occurred, necessitating five intrauterine transfusions to ultimately correct the fetal anemia. Conclusions The use of a smaller-diameter procedure needle, correction of the fetal thrombocytopenia early in the procedure, and external cord compression with the ultrasound transducer were ultimately successful measures in allowing for minimal loss of transfused red cells from the intravascular compartment.
引言 胎儿失血是脐带穿刺术的一种罕见并发症。成功纠正胎儿血小板减少症对于降低风险至关重要。病例报告 一名25岁、孕3产2(0-0-0-2)的孕妇,在妊娠27周时因评估新诊断的细小病毒感染继发的非免疫性水肿而转诊。尽管使用辅助性血小板输注来纠正严重的胎儿血小板减少症,但脐带穿刺部位仍持续出血,需要进行五次宫内输血才能最终纠正胎儿贫血。结论 使用较小直径的操作针、在操作早期纠正胎儿血小板减少症以及用超声换能器进行脐带外部压迫,最终成功地减少了血管内输注的红细胞的损失。