Health Challenges and Systems, African Population and Health Research Center, Nairobi, Kenya; Department of Global Health, Amsterdam Institute for Global Health and Development, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands;
Glob Health Action. 2013 Oct 21;6:22510. doi: 10.3402/gha.v6i0.22510.
Cardiovascular disease (CVD) is a leading cause of death in sub-Saharan Africa (SSA), with annual deaths expected to increase to 2 million by 2030. Currently, most national health systems in SSA are not adequately prepared for this epidemic. This is especially so in slum settlements where access to formal healthcare and resources is limited.
To develop and introduce a model of cardiovascular prevention in the slums of Nairobi by integrating public health and private sector approaches.
Two non-profit organizations that conduct public health research, Amsterdam Institute for Global Health and Development (AIGHD) and African Population and Health Research Center (APHRC), collaborated with private-sector Boston Consulting Group (BCG) to develop a service delivery package for CVD prevention in slum settings. A theoretic model was designed based on the integration of public and private sector approaches with the focus on costs and feasibility.
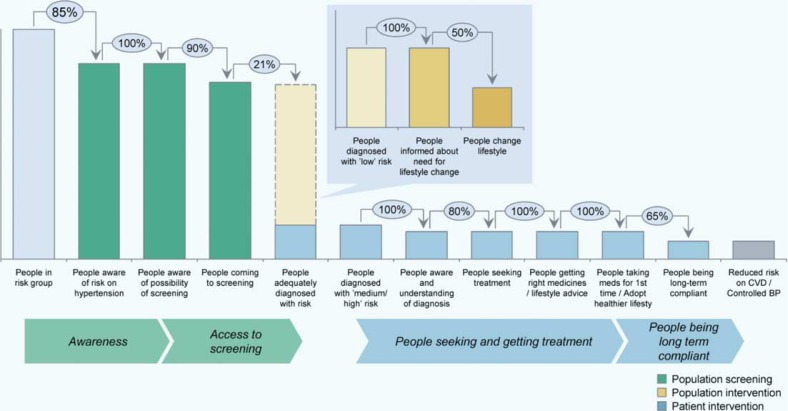
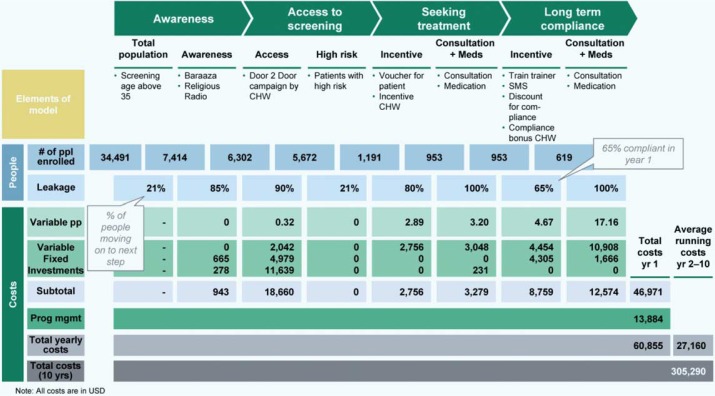
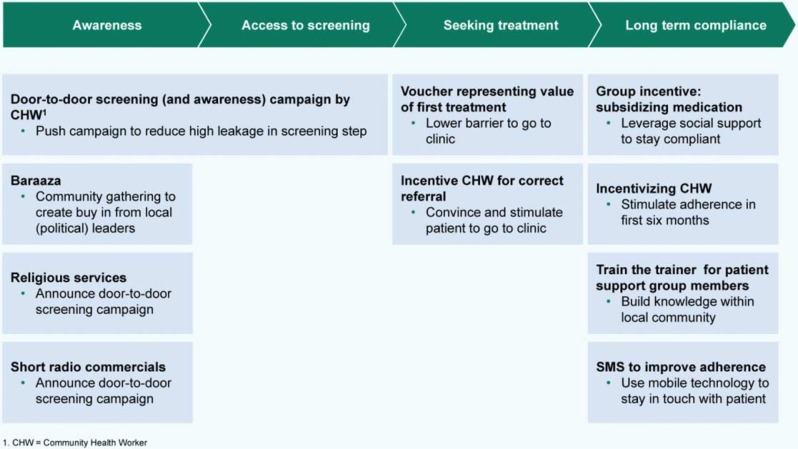
The final model includes components that aim to improve community awareness, a home-based screening service, patient and provider incentives to seek and deliver treatment specifically for hypertension, and adherence support. The expected outcomes projected by this model could prove potentially cost effective and affordable (1 USD/person/year). The model is currently being implemented in a Nairobi slum and is closely followed by key stakeholders in Kenya including the Ministry of Health, the World Health Organization (WHO), and leading non-governmental organizations (NGOs).
Through the collaboration of public health and private sectors, a theoretically cost-effective model was developed for the prevention of CVD and is currently being implemented in the slums of Nairobi. If results are in line with the theoretical projections and first impressions on the ground, scale-up of the service delivery package could be planned in other poor urban areas in Kenya by relevant policymakers and NGOs.
心血管疾病(CVD)是撒哈拉以南非洲(SSA)的主要死亡原因,预计到 2030 年,每年的死亡人数将增加到 200 万。目前,SSA 的大多数国家卫生系统对此类流行病没有充分的准备。在贫民窟,这种情况尤其如此,因为那里获得正规医疗保健和资源的机会有限。
通过整合公共卫生和私营部门的方法,在肯尼亚内罗毕的贫民窟中建立和引入心血管疾病预防模式。
两家从事公共卫生研究的非营利组织,即阿姆斯特丹全球健康与发展研究所(AIGHD)和非洲人口与健康研究中心(APHRC),与私营部门波士顿咨询集团(BCG)合作,为贫民窟环境中的 CVD 预防制定了服务提供方案。该理论模型是基于公共和私营部门方法的整合而设计的,重点是成本和可行性。
最终模型包括旨在提高社区意识、家庭为基础的筛查服务、患者和提供者激励措施以寻求和提供专门针对高血压的治疗以及坚持支持的组成部分。该模型预计的结果可能具有潜在的成本效益和负担能力(每人每年 1 美元)。该模型目前正在内罗毕的一个贫民窟中实施,并受到肯尼亚的利益攸关方(包括卫生部、世界卫生组织(世卫组织)和主要非政府组织(NGO))的密切关注。
通过公共卫生和私营部门的合作,为 CVD 的预防制定了一种理论上具有成本效益的模式,目前正在内罗毕的贫民窟中实施。如果结果符合理论预测和实地的初步印象,相关政策制定者和非政府组织可以计划在肯尼亚其他贫困城市地区扩大服务提供方案。