van de Vijver Steven, Oti Samuel, Moll van Charante Eric, Allender Steven, Foster Charlie, Lange Joep, Oldenburg Brian, Kyobutungi Catherine, Agyemang Charles
African Population and Health Research Center, Nairobi, Kenya.
Department of Global Health, Academic Medical Center, Amsterdam Institute for Global Health and Development, University of Amsterdam, Amsterdam, The Netherlands.
Global Health. 2015 Mar 7;11:11. doi: 10.1186/s12992-015-0095-y.
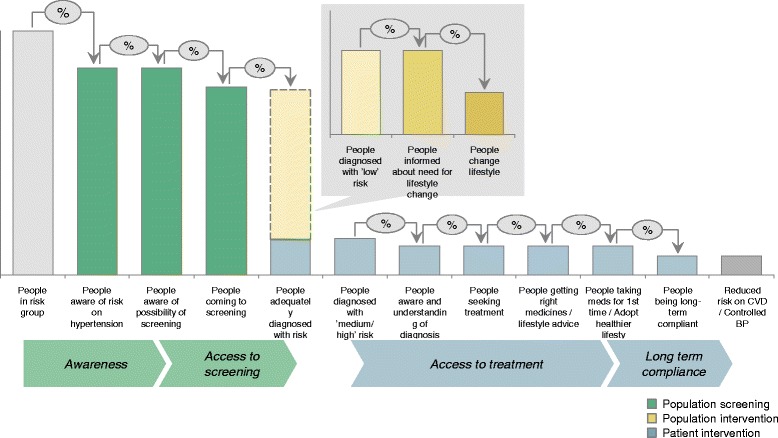
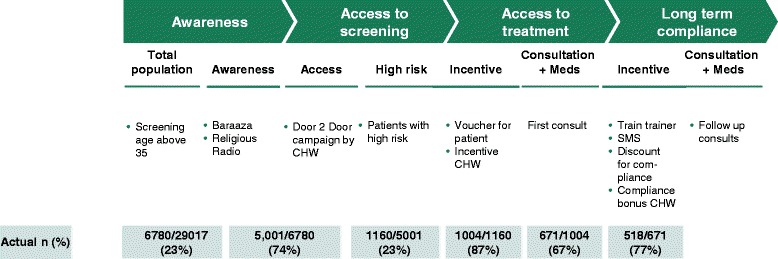
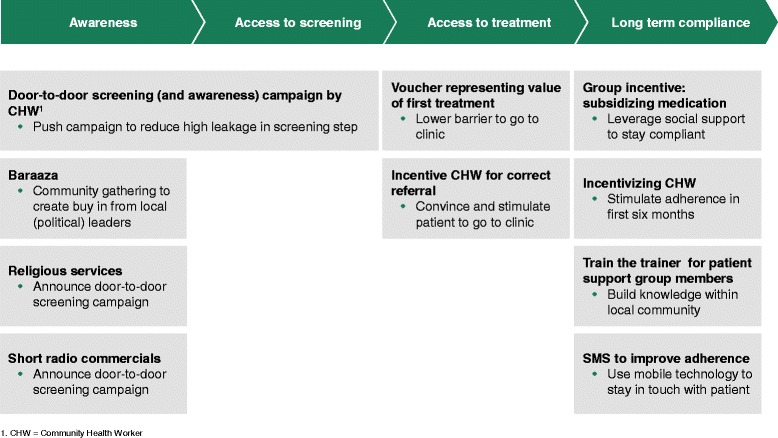
Cardiovascular diseases (CVD) are the main cause of morbidity and mortality worldwide. As prevention and treatment of CVD often requires active screening and lifelong follow up it is a challenge for health systems both in high-income and low and middle-income countries to deliver adequate care to those in need, with efficient use of resources.We developed a health service model for primary prevention of CVD suitable for implementation in the Nairobi slums, based on best practices from public health and the private sectors. The model consists of four key intervention elements focusing on increasing awareness, incentives for promoting access to screening and treatment, and improvement of long-term adherence to prescribed medications. More than 5,000 slum dwellers aged ≥35 years and above have been screened in the study resulting in more than 1000 diagnosed with hypertension and referred to the clinic.Some marginalized groups in high-income countries like African migrants in the Netherlands also have low rates of awareness, treatment and control of hypertension as the slum population in Nairobi. The parallel between both groups is that they have a combination of risky lifestyle, are prone to chronic diseases such as hypertension, have limited knowledge about hypertension and its complications, and a tendency to stay away from clinics partly due to cultural beliefs in alternative forms of treatment, and lack of trust in health providers. Based on these similarities it was suggested by several policymakers that the model from Nairobi can be applied to other vulnerable populations such as African migrants in high-income countries. The model can be contextualized to the local situation by adapting the key steps of the model to the local settings.The involvement and support of African communities' infrastructures and health care staff is crucial, and the most important enabler for successful implementation of the model in migrant communities in high-income countries. Once these stakeholders have expressed their interest, the impact of the adapted intervention can be measured through an implementation research approach including collection of costs from health care providers' perspective and health effects in the target population, similar to the study design for Nairobi.
心血管疾病(CVD)是全球发病和死亡的主要原因。由于心血管疾病的预防和治疗通常需要积极筛查和终身随访,因此无论是高收入国家还是低收入和中等收入国家的卫生系统,要为有需要的人提供充分的护理并有效利用资源都是一项挑战。我们基于公共卫生和私营部门的最佳实践,开发了一种适用于在内罗毕贫民窟实施的心血管疾病一级预防卫生服务模式。该模式由四个关键干预要素组成,重点是提高认识、激励人们接受筛查和治疗,以及改善对处方药的长期依从性。在这项研究中,对5000多名35岁及以上的贫民窟居民进行了筛查,结果发现1000多人被诊断患有高血压并被转诊至诊所。在高收入国家,一些边缘化群体,如荷兰的非洲移民,其高血压的知晓率、治疗率和控制率也与内罗毕的贫民窟人口一样低。这两类人群的相似之处在于,他们都有不良生活方式,易患高血压等慢性病,对高血压及其并发症的了解有限,部分由于对替代治疗形式的文化信仰以及对医疗服务提供者缺乏信任而不愿去诊所。基于这些相似之处,几位政策制定者建议,内罗毕的模式可以应用于其他弱势群体,如高收入国家的非洲移民。通过使该模式的关键步骤适应当地情况,可以将该模式因地制宜。非洲社区基础设施和医护人员的参与和支持至关重要,这是该模式在高收入国家移民社区成功实施的最重要推动因素。一旦这些利益相关者表达了他们的兴趣,就可以通过实施研究方法来衡量适应性干预的影响,包括从医疗服务提供者的角度收集成本以及目标人群的健康效果,这与内罗毕的研究设计类似。