Melbourne School of Psychological Sciences, University of Melbourne, Melbourne, Victoria, Australia.
PLoS One. 2013 Nov 1;8(11):e78286. doi: 10.1371/journal.pone.0078286. eCollection 2013.
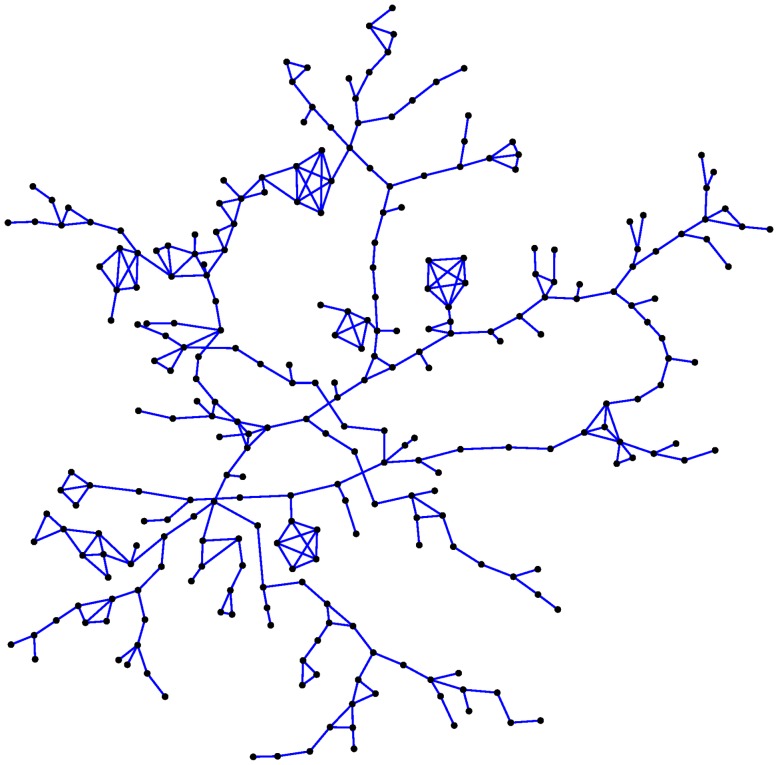
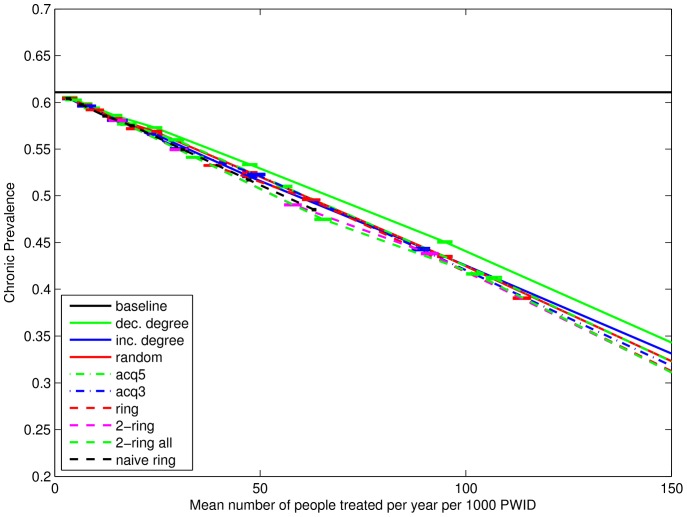
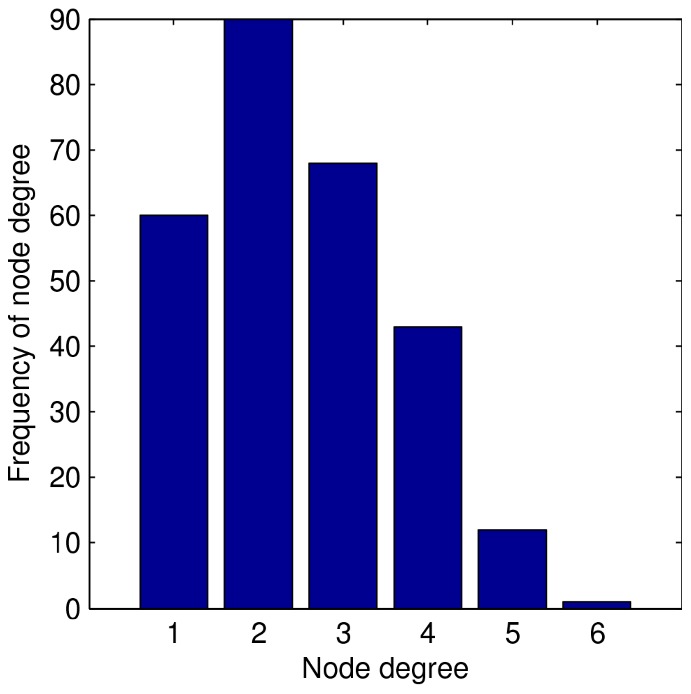
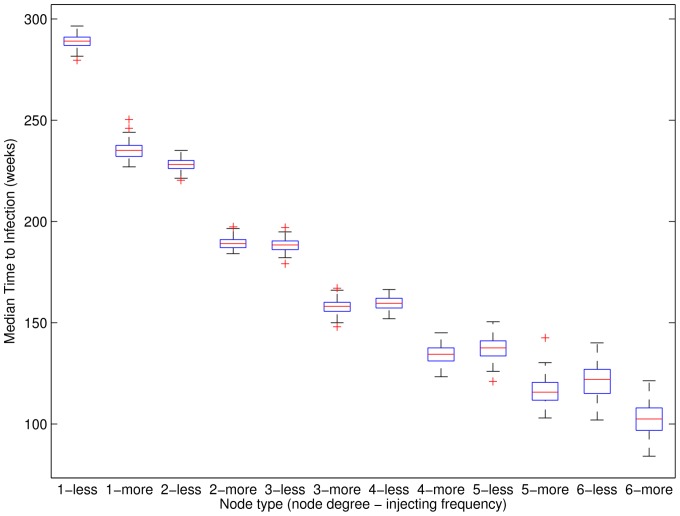
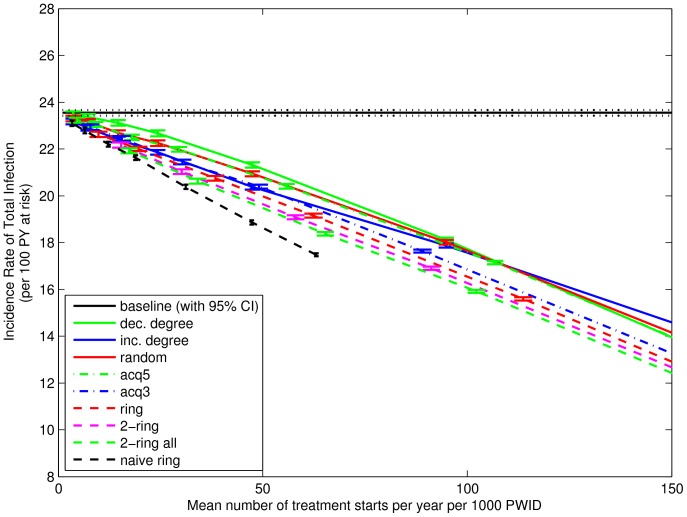
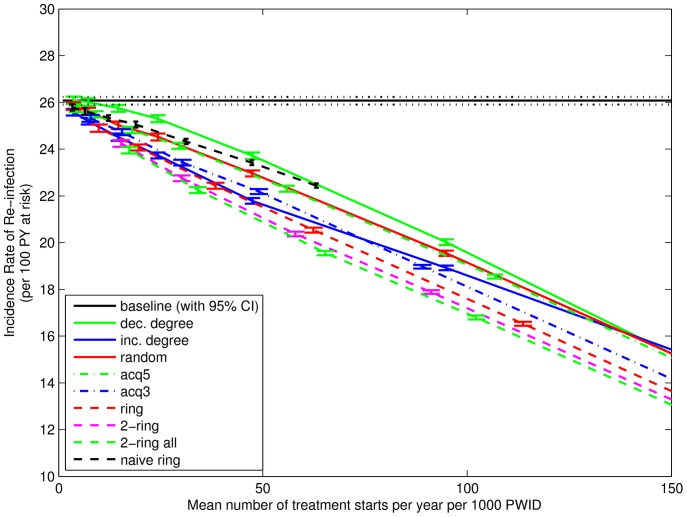
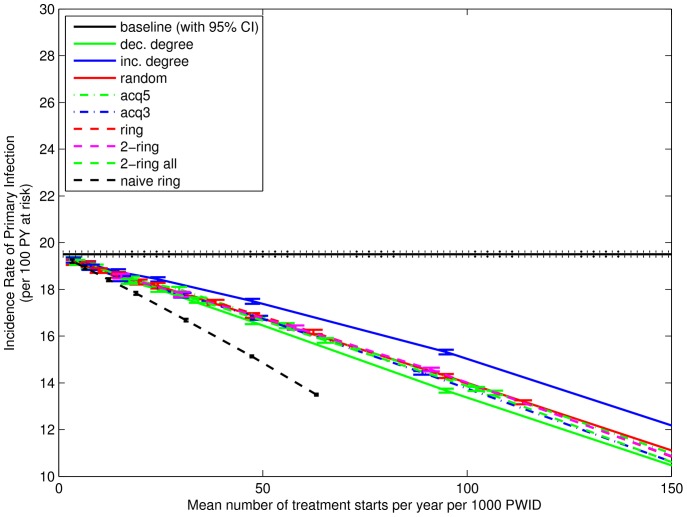
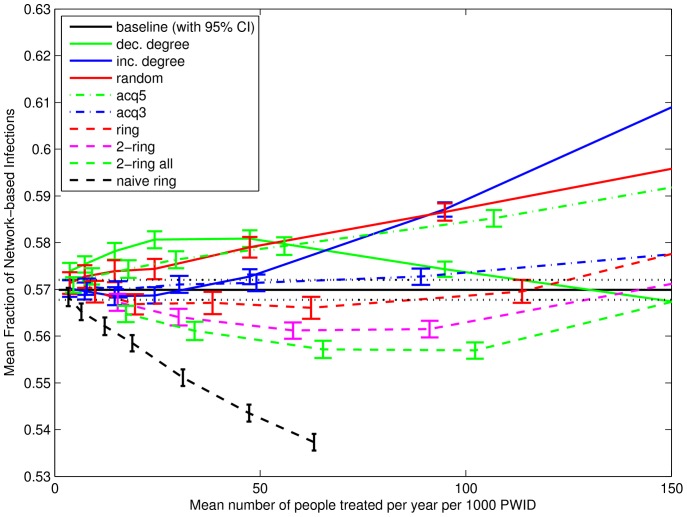
Hepatitis C virus (HCV) chronically infects over 180 million people worldwide, with over 350,000 estimated deaths attributed yearly to HCV-related liver diseases. It disproportionally affects people who inject drugs (PWID). Currently there is no preventative vaccine and interventions feature long treatment durations with severe side-effects. Upcoming treatments will improve this situation, making possible large-scale treatment interventions. How these strategies should target HCV-infected PWID remains an important unanswered question. Previous models of HCV have lacked empirically grounded contact models of PWID. Here we report results on HCV transmission and treatment using simulated contact networks generated from an empirically grounded network model using recently developed statistical approaches in social network analysis. Our HCV transmission model is a detailed, stochastic, individual-based model including spontaneously clearing nodes. On transmission we investigate the role of number of contacts and injecting frequency on time to primary infection and the role of spontaneously clearing nodes on incidence rates. On treatment we investigate the effect of nine network-based treatment strategies on chronic prevalence and incidence rates of primary infection and re-infection. Both numbers of contacts and injecting frequency play key roles in reducing time to primary infection. The change from "less-" to "more-frequent" injector is roughly similar to having one additional network contact. Nodes that spontaneously clear their HCV infection have a local effect on infection risk and the total number of such nodes (but not their locations) has a network wide effect on the incidence of both primary and re-infection with HCV. Re-infection plays a large role in the effectiveness of treatment interventions. Strategies that choose PWID and treat all their contacts (analogous to ring vaccination) are most effective in reducing the incidence rates of re-infection and combined infection. A strategy targeting infected PWID with the most contacts (analogous to targeted vaccination) is the least effective.
丙型肝炎病毒 (HCV) 在全球范围内慢性感染超过 1.8 亿人,每年估计有超过 35 万人因 HCV 相关肝病而死亡。它不成比例地影响到注射毒品者(PWID)。目前尚无预防性疫苗,干预措施的特点是治疗时间长,副作用严重。即将推出的治疗方法将改善这种情况,从而实现大规模的治疗干预。这些策略应该如何针对 HCV 感染的 PWID 仍然是一个重要的未解决问题。以前的 HCV 模型缺乏基于经验的 PWID 接触模型。在这里,我们报告了使用最近开发的社交网络分析中的统计方法从基于经验的网络模型生成的模拟接触网络来研究 HCV 传播和治疗的结果。我们的 HCV 传播模型是一个详细的、随机的、基于个体的模型,包括自发清除节点。在传播方面,我们研究了接触次数和注射频率对原发性感染时间的作用,以及自发清除节点对发病率的作用。在治疗方面,我们研究了九种基于网络的治疗策略对慢性流行率和原发性感染及再感染发生率的影响。接触次数和注射频率都在减少原发性感染时间方面发挥着关键作用。从“较少”到“更频繁”的注射者的转变大致类似于增加一个网络接触者。自发清除 HCV 感染的节点对感染风险有局部影响,而这些节点的总数(但不是它们的位置)对原发性和再感染 HCV 的总发病率都有网络影响。再感染在治疗干预的有效性中起着重要作用。选择 PWID 并治疗其所有接触者的策略(类似于环状疫苗接种)在降低再感染和合并感染的发生率方面最为有效。针对接触者最多的感染 PWID 的策略(类似于靶向疫苗接种)效果最差。