Department of Internal Medicine Faculty of Medicine, Padjadjaran University/Hasan Sadikin Hospital, Bandung, Indonesia ; Health Research Unit, Faculty of Medicine, Padjadjaran University, Bandung, Indonesia.
PLoS One. 2013 Nov 11;8(11):e79904. doi: 10.1371/journal.pone.0079904. eCollection 2013.
Distortion of iron homeostasis may contribute to the pathogenesis of human immunodeficiency virus (HIV) infection and tuberculosis (TB). We studied the association of the central iron-regulatory hormone hepcidin with the severity of HIV and the association between hepcidin and other markers of iron homeostasis with development of TB.
Three groups of patients were selected from a prospective cohort of HIV-infected subjects in Bandung, Indonesia. The first group consisted of HIV-infected patients who started TB treatment more than 30 days after cohort enrollment (cases). The second group consisted of HIV-infected patients who were matched for age, gender and CD4 cell count to the cases group (matched controls). The third group consisted of HIV-infected patients with CD4 cell counts above 200 cells/mm(3) (unmatched controls). Iron parameters including hepcidin were compared using samples collected at cohort enrollment, and compared with recently published reference values for serum hepcidin.
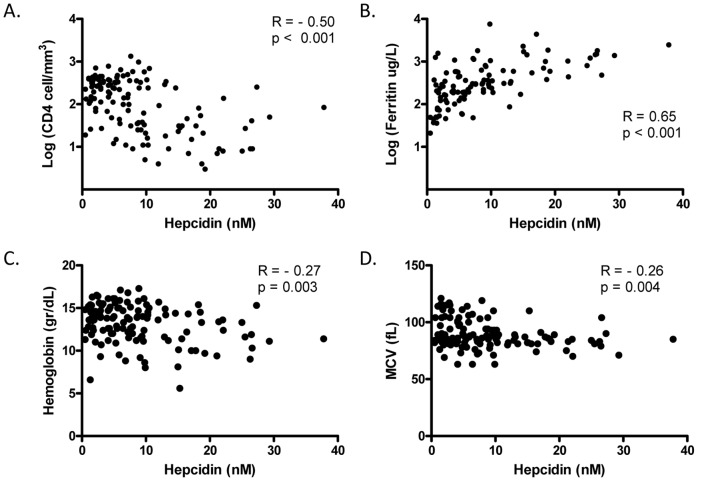
A total of 127 HIV-infected patients were included, 42 cases together with 42 matched controls and 43 unmatched controls. Patients with advanced HIV infection had elevated serum hepcidin and ferritin levels. Hepcidin levels correlated inversely with CD4 cells and hemoglobin. Cases had significantly higher hepcidin and ferritin concentrations at cohort enrollment compared to matched controls, but these differences were fully accounted for by the cases who started TB treatment between day 31 and 60 after enrollment. Hepcidin levels were not different in those with or without hepatitis C infection.
Iron metabolism is distorted in advanced HIV infection with CD4 cell counts correlating inversely with serum hepcidin levels. High serum hepcidin levels and hyperferritinemia were found in patients starting TB treatment shortly after cohort enrollment, suggesting that these parameters have a predictive value for development of manifest TB in HIV-infected patients.
铁稳态的紊乱可能导致人类免疫缺陷病毒(HIV)感染和结核病(TB)的发病机制。我们研究了中枢铁调节激素铁调素与 HIV 严重程度的关系,以及铁调素与其他铁稳态标志物之间的关系与 TB 的发生。
从印度尼西亚万隆的 HIV 感染患者前瞻性队列中选择了三组患者。第一组为队列入组后 30 天以上开始 TB 治疗的 HIV 感染患者(病例)。第二组为与病例组年龄、性别和 CD4 细胞计数相匹配的 HIV 感染患者(匹配对照组)。第三组为 CD4 细胞计数大于 200 个/mm(3)的 HIV 感染患者(未匹配对照组)。使用队列入组时采集的样本比较铁参数,包括铁调素,并与最近发表的血清铁调素参考值进行比较。
共纳入 127 例 HIV 感染患者,其中 42 例病例,42 例匹配对照,43 例未匹配对照。晚期 HIV 感染患者的血清铁调素和铁蛋白水平升高。铁调素水平与 CD4 细胞和血红蛋白呈负相关。病例组在队列入组时的铁调素和铁蛋白浓度明显高于匹配对照组,但这些差异完全由入组后第 31 至 60 天开始接受 TB 治疗的病例引起。有无丙型肝炎感染的患者铁调素水平无差异。
CD4 细胞计数与血清铁调素水平呈负相关,晚期 HIV 感染时铁代谢紊乱。在队列入组后不久开始接受 TB 治疗的患者中,发现血清铁调素水平高和铁蛋白血症,表明这些参数对 HIV 感染患者发生显性 TB 具有预测价值。