Rajaratnam Bala S, Goh James Ch, Kumar Prem V
School of Health Sciences (Allied Health), Nanyang Polytechnic, 180 Ang Mo Kio Avenue 8, 569830, Singapore.
BMC Sports Sci Med Rehabil. 2013 Dec 6;5(1):26. doi: 10.1186/2052-1847-5-26.
Muscles are important "sensors of the joint instability". The aim of this study was to identify the neuro-motor control strategies adopted by patients with anterior shoulder instability during overhead shoulder elevation in two planes.
The onset, time of peak activation, and peak magnitude of seven shoulder muscles (posterior deltoid, bilateral upper trapezius, biceps brachii, infraspinatus, supraspinatus and teres major) were identified using electromyography as 19 pre-operative patients with anterior shoulder instability (mean 27.95 years, SD = 7.796) and 25 age-matched asymptomatic control subjects (mean 23.07 years, SD = 2.952) elevated their arm above 90 degrees in the sagittal and coronal planes.
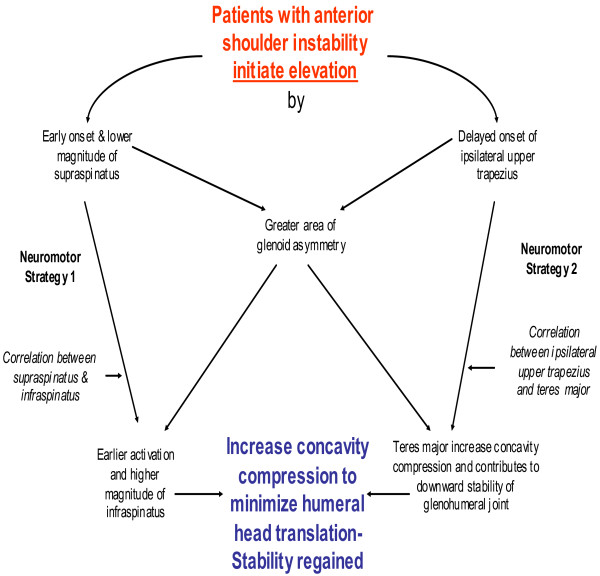
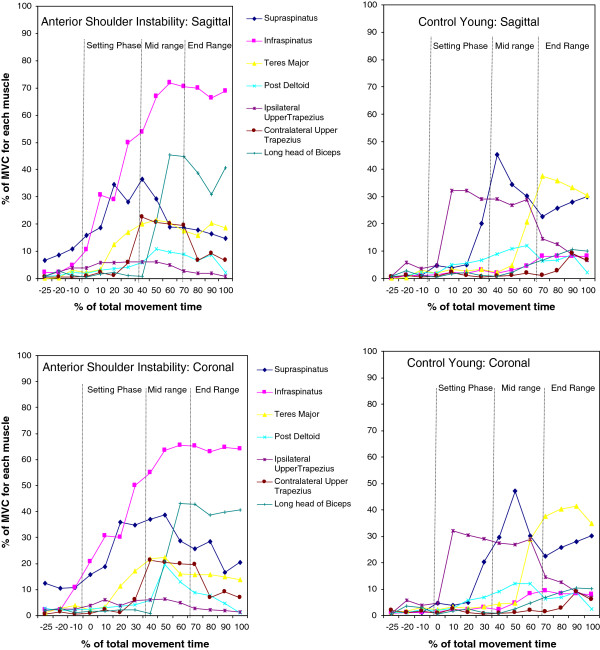
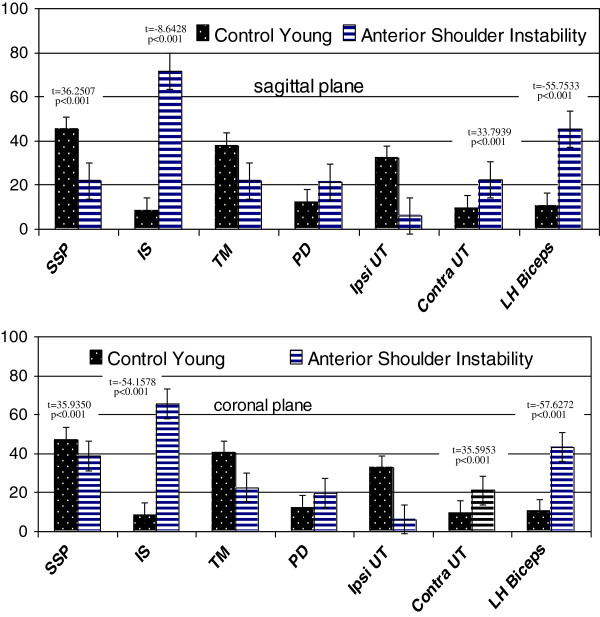
Temporal characteristics of time of muscle onsets were significantly different between groups expect for teres major in the coronal plane (t = 1.1220, p = 0.2646) Patients recruited the rotator cuff muscles earlier and delayed the onset of ipsilateral upper trapezius compared with subjects (p<0.001) that control subjects. Furthermore, significant alliances existed between the onsets of infraspinatus and supraspinatus (sagittal: r = 0.720; coronal: r = 0.756 at p<0.001) and ipsilateral upper trapezius and infraspinatus (sagittal: r = -0.760, coronal: r = -0.818 at p<0.001). The peak activation of all seven muscles occurred in the mid-range of elevation among patients with anterior shoulder instability whereas subjects spread peak activation of all 7 muscles throughout range. Peak magnitude of patients' infraspinatus muscle was six times higher (sagittal: t = -8.6428, coronal: t = -54.1578 at p<0.001) but magnitude of their supraspinatus was lower (sagittal: t = 36.2507, coronal: t = 35.9350 at p<0.001) that subjects.
Patients with anterior shoulder instability adopted a "stability before mobility" neuro-motor control strategy to initiate elevation and a "stability at all cost" strategy to ensure concavity compression in the mid-to-150 degrees of elevation in both sagittal and coronal planes.
肌肉是重要的“关节不稳定传感器”。本研究的目的是确定前肩不稳患者在两个平面进行过顶肩抬高时所采用的神经运动控制策略。
使用肌电图确定19例术前前肩不稳患者(平均27.95岁,标准差=7.796)和25例年龄匹配的无症状对照受试者(平均23.07岁,标准差=2.952)在矢状面和冠状面将手臂抬高超过90度时,七块肩部肌肉(后三角肌、双侧上斜方肌、肱二头肌、冈下肌、冈上肌和大圆肌)的起始时间、峰值激活时间和峰值大小。
除冠状面的大圆肌外(t = 1.1220,p = 0.2646),两组之间肌肉起始时间的时间特征存在显著差异。与对照受试者相比,患者更早募集肩袖肌群,并延迟同侧上斜方肌的起始时间(p<0.001)。此外,冈下肌和冈上肌的起始时间之间存在显著相关性(矢状面:r = 0.720;冠状面:r = 0.756,p<0.001),同侧上斜方肌和冈下肌的起始时间之间也存在显著相关性(矢状面:r = -0.760,冠状面:r = -0.818,p<0.001)。在前肩不稳患者中,所有七块肌肉的峰值激活均出现在抬高的中间范围,而对照受试者的七块肌肉的峰值激活则分布在整个范围内。患者冈下肌的峰值大小比对照受试者高六倍(矢状面:t = -8.6428,冠状面:t = -54.1578,p<0.001),但其冈上肌的大小则低于对照受试者(矢状面:t = 36.2507,冠状面:t = 35.9350,p<0.001)。
前肩不稳患者采用“先稳定后活动”的神经运动控制策略来启动抬高,并采用“不惜一切代价保持稳定”的策略来确保在矢状面和冠状面抬高至150度的过程中凹面压缩。