Department of Infectious Diseases, The Third Hospital of Hebei Medical University, Shijiazhuang, China.
PLoS One. 2013 Dec 4;8(12):e82092. doi: 10.1371/journal.pone.0082092. eCollection 2013.
Nonalcoholic fatty liver disease (NAFLD) is one of the critical public health problems in China. The full spectrum of the disease ranges from simple steatosis and nonalcoholic steatohepatitis (NASH) to cirrhosis and hepatocellular carcinoma(HCC). The infiltration of inflammatory cells characterizes NASH. This characteristic contributes to the progression of hepatitis, fibrosis, cirrhosis, and HCC. Therefore, distinguishing NASH from NAFLD is crucial.
Ninety-five patients with NAFLD, 44 with NASH, and 51 with non-NASH were included in the study to develop a new scoring system for differentiating NASH from NAFLD. Data on clinical and biological characteristics, as well as blood information, were obtained. Cytokeratin-18 (CK-18) fragments levels were measured using an enzyme-linked immunosorbant assay.
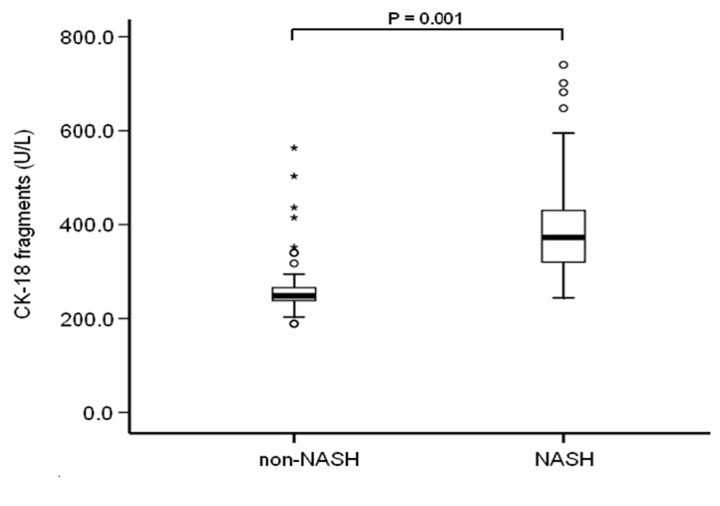
Several indexes show significant differences between the two groups, which include body mass index (BMI), waist-on-hip ratio (WHR), aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), γ-glutamyl transpeptidase (γ-GT), platelets, uric acid (UA), hs-C-reactive protein (hs-CRP), triglycerides (TG), albumin (ALB), and CK-18 fragments (all P < 0.05). The CK-18 fragment levels showed a significant positive correlation with steatosis severity, ballooning, lobular inflammation, and fibrosis stage (all P < 0.05). Therefore, a new model that combines ALT, platelets, CK-18 fragments, and TG was established by logistic regression among NAFLD patients. The AUROC curve in predicting NASH was 0.920 (95% CI: 0.866 - 0.974, cutoff value = 0.361, sensitivity = 89%, specificity = 86%, positive predictive value = 89%, negative predictive value = 89%).
The novel scoring system may be considered as a useful model in predicting the presence of NASH in NAFLD patients.
非酒精性脂肪性肝病(NAFLD)是中国重要的公共卫生问题之一。该疾病谱从单纯性脂肪变性和非酒精性脂肪性肝炎(NASH)到肝硬化和肝细胞癌(HCC)不等。炎症细胞浸润是 NASH 的特征。这种特征导致肝炎、纤维化、肝硬化和 HCC 的进展。因此,区分 NASH 与 NAFLD 非常重要。
本研究纳入 95 例 NAFLD 患者、44 例 NASH 患者和 51 例非 NASH 患者,旨在建立一种新的评分系统,以区分 NASH 与 NAFLD。收集临床和生物学特征以及血液信息。采用酶联免疫吸附试验检测细胞角蛋白 18(CK-18)片段水平。
两组间多项指标存在显著差异,包括体重指数(BMI)、腰臀比(WHR)、天门冬氨酸氨基转移酶(AST)、丙氨酸氨基转移酶(ALT)、碱性磷酸酶(ALP)、γ-谷氨酰转肽酶(γ-GT)、血小板、尿酸(UA)、高敏 C 反应蛋白(hs-CRP)、三酰甘油(TG)、白蛋白(ALB)和 CK-18 片段(均 P<0.05)。CK-18 片段水平与脂肪变性严重程度、气球样变、肝小叶炎症和纤维化分期呈显著正相关(均 P<0.05)。因此,通过对 NAFLD 患者进行 logistic 回归分析,建立了一种由 ALT、血小板、CK-18 片段和 TG 组成的新模型。预测 NASH 的 AUROC 曲线为 0.920(95%CI:0.866-0.974,截断值=0.361,敏感度=89%,特异度=86%,阳性预测值=89%,阴性预测值=89%)。
新型评分系统可作为预测 NAFLD 患者 NASH 存在的有用模型。