Boriani Giuseppe, Glotzer Taya V, Santini Massimo, West Teena M, De Melis Mirko, Sepsi Milan, Gasparini Maurizio, Lewalter Thorsten, Camm John A, Singer Daniel E
Department of Experimental, Diagnostic and Specialty Medicine, Institute of Cardiology, University of Bologna, S.Orsola-Malpighi University Hospital, Via Massarenti 9, Bologna 40138, Italy.
Eur Heart J. 2014 Feb;35(8):508-16. doi: 10.1093/eurheartj/eht491. Epub 2013 Dec 11.
The aim of this study was to assess the association between maximum daily atrial fibrillation (AF) burden and risk of ischaemic stroke.
Cardiac implanted electronic devices (CIEDs) enhance detection of AF, providing a comprehensive measure of AF burden.
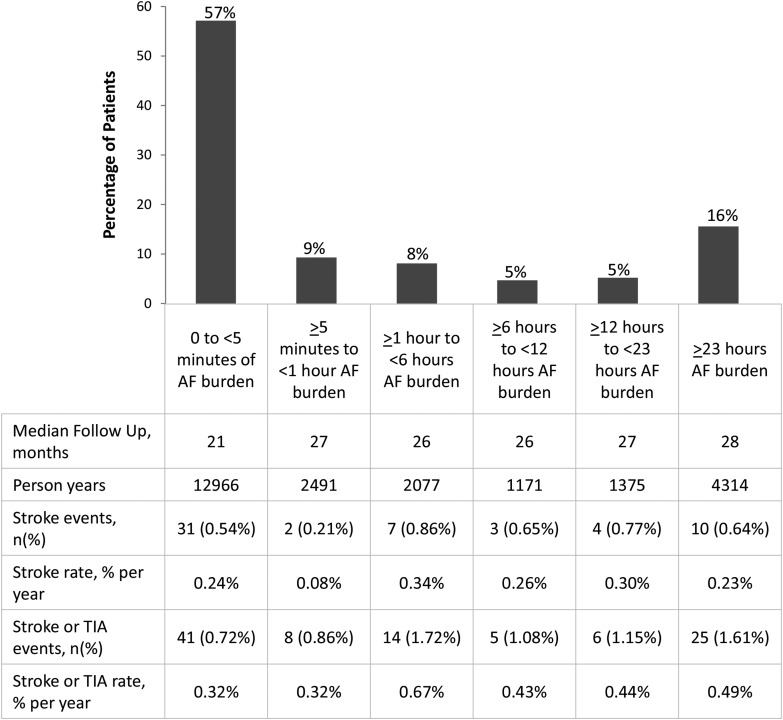
DESIGN, SETTING, AND PATIENTS: A pooled analysis of individual patient data from five prospective studies was performed. Patients without permanent AF, previously implanted with CIEDs, were included if they had at least 3 months of follow-up. A total of 10 016 patients (median age 70 years) met these criteria. The risk of ischaemic stroke associated with pre-specified cut-off points of AF burden (5 min, 1, 6, 12, and 23 h, respectively) was assessed.
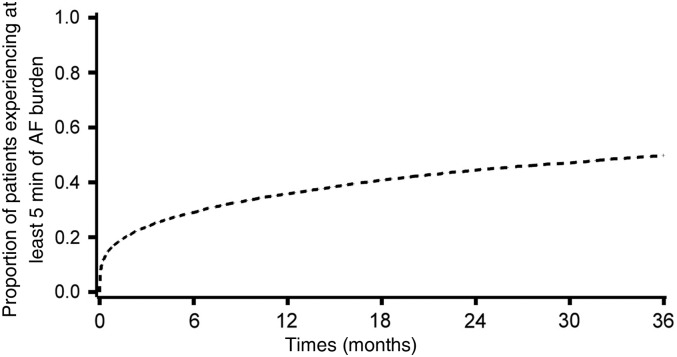
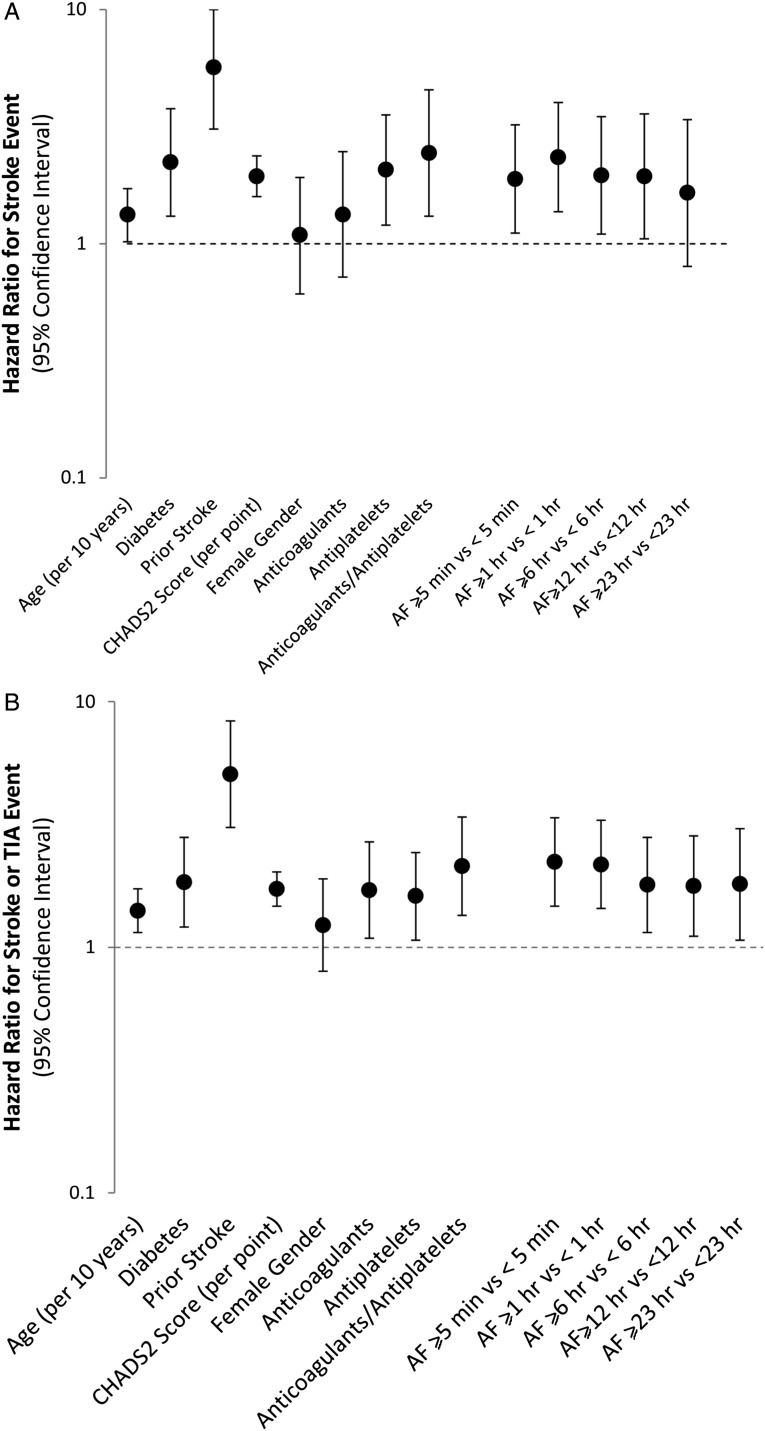
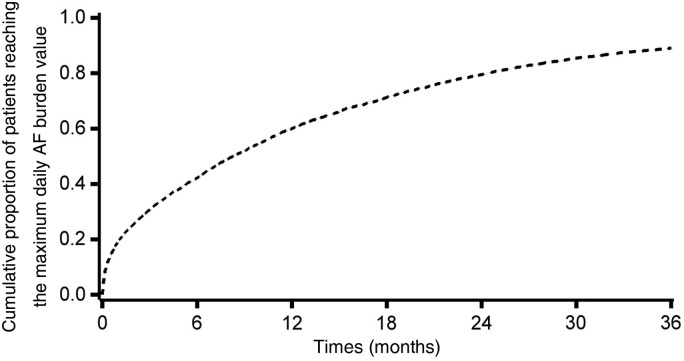
During a median follow-up of 24 months, 43% of 10 016 patients experienced at least 1 day with at least 5 min of AF burden and for them the median time to the maximum AF burden was 6 months (inter-quartile range: 1.3-14). A Cox regression analysis adjusted for the CHADS2 score and anticoagulants at baseline demonstrated that AF burden was an independent predictor of ischaemic stroke. Among the thresholds of AF burden that we evaluated, 1 h was associated with the highest hazard ratio (HR) for ischaemic stroke, i.e. 2.11 (95% CI: 1.22-3.64, P = 0.008).
Device-detected AF burden is associated with an increased risk of ischaemic stroke in a relatively unselected population of CIEDs patients. This finding may add to the basis for timely and clinically appropriate decision-making on anticoagulation treatment.
本研究旨在评估每日最大房颤(AF)负荷与缺血性卒中风险之间的关联。
心脏植入式电子设备(CIEDs)可增强房颤检测能力,提供房颤负荷的综合测量指标。
设计、研究地点和患者:对五项前瞻性研究的个体患者数据进行汇总分析。纳入既往植入CIEDs且无永久性房颤的患者,条件是他们至少有3个月的随访期。共有10016名患者(中位年龄70岁)符合这些标准。评估了与预先设定的房颤负荷截断点(分别为5分钟、1小时、6小时、12小时和23小时)相关的缺血性卒中风险。
在中位随访24个月期间,10016名患者中有43%经历过至少1天房颤负荷至少5分钟,其中位达到最大房颤负荷的时间为6个月(四分位间距:1.3 - 14)。校正基线CHADS2评分和抗凝剂使用情况后的Cox回归分析表明,房颤负荷是缺血性卒中的独立预测因素。在我们评估的房颤负荷阈值中,1小时与缺血性卒中的最高风险比(HR)相关,即2.11(95%置信区间:1.22 - 3.64,P = 0.008)。
在相对未经过筛选的CIEDs患者群体中,设备检测到的房颤负荷与缺血性卒中风险增加相关。这一发现可能为抗凝治疗的及时和临床适当决策提供更多依据。