First Critical Care Department, National and Kapodistrian University of Athens School of Medicine, Evangelismos General Hospital, Ypsilantou 45-47, Athens 106 75, Greece.
Ann Intensive Care. 2013 Dec 19;3(1):39. doi: 10.1186/2110-5820-3-39.
Intensive care unit-acquired weakness (ICUAW) is a common complication, associated with significant morbidity. Neuromuscular electrical stimulation (NMES) has shown promise for prevention. NMES acutely affects skeletal muscle microcirculation; such effects could mediate the favorable outcomes. However, optimal current characteristics have not been defined. This study aimed to compare the effects on muscle microcirculation of a single NMES session using medium and high frequency currents.
ICU patients with systemic inflammatory response syndrome (SIRS) or sepsis of three to five days duration and patients with ICUAW were studied. A single 30-minute NMES session was applied to the lower limbs bilaterally using current of increasing intensity. Patients were randomly assigned to either the HF (75 Hz, pulse 400 μs, cycle 5 seconds on - 21 seconds off) or the MF (45 Hz, pulse 400 μs, cycle 5 seconds on - 12 seconds off) protocol. Peripheral microcirculation was monitored at the thenar eminence using near-infrared spectroscopy (NIRS) to obtain tissue O2 saturation (StO2); a vascular occlusion test was applied before and after the session. Local microcirculation of the vastus lateralis was also monitored using NIRS.
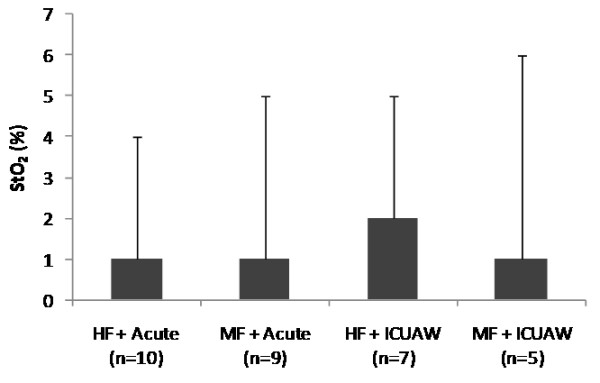
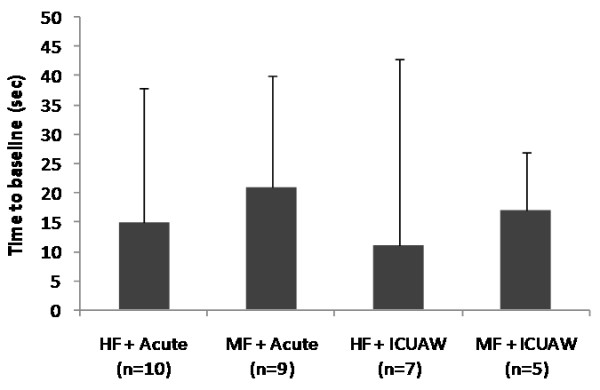
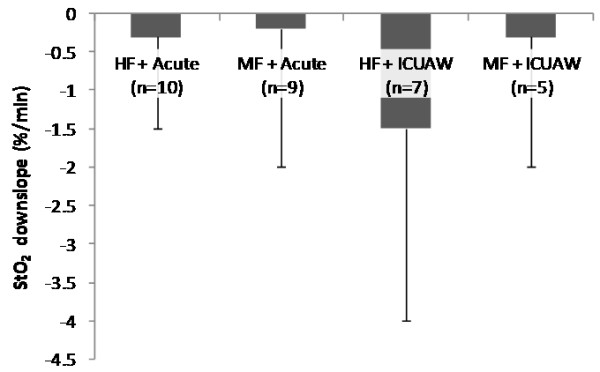
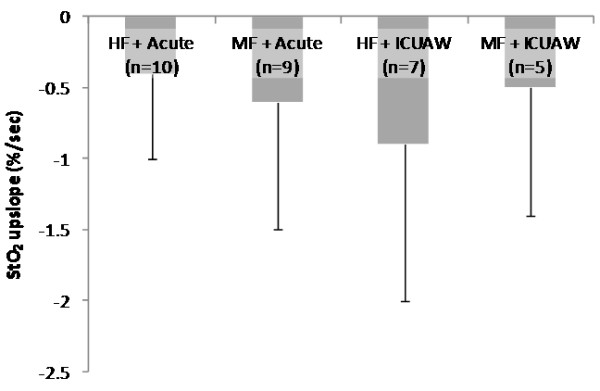
Thirty-one patients were randomized. In the HF protocol (17 patients), peripheral microcirculatory parameters were: thenar O2 consumption rate (%/minute) from 8.6 ± 2.2 to 9.9 ± 5.1 (P = 0.08), endothelial reactivity (%/second) from 2.7 ± 1.4 to 3.2 ± 1.9 (P = 0.04), vascular reserve (seconds) from 160 ± 55 to 145 ± 49 (P = 0.03). In the MF protocol: thenar O2 consumption rate (%/minute) from 8.8 ± 3.8 to 9.9 ± 3.6 (P = 0.07), endothelial reactivity (%/second) from 2.5 ± 1.4 to 3.1 ± 1.7 (P = 0.03), vascular reserve (seconds) from 163 ± 37 to 144 ± 33 (P = 0.001). Both protocols showed a similar effect. In the vastus lateralis, average muscle O2 consumption rate was 61 ± 9%/minute during the HF protocol versus 69 ± 23%/minute during the MF protocol (P = 0.5). The minimum amplitude in StO2 was 5 ± 4 units with the HF protocol versus 7 ± 4 units with the MF protocol (P = 0.3). Post-exercise, StO2 increased by 6 ± 7 units with the HF protocol versus 5 ± 4 units with the MF protocol (P = 0.6). These changes correlated well with contraction strength.
A single NMES session affected local and systemic skeletal muscle microcirculation. Medium and high frequency currents were equally effective.
重症监护病房获得性肌无力(ICUAW)是一种常见的并发症,与显著的发病率相关。神经肌肉电刺激(NMES)已显示出预防作用的潜力。NMES 急性影响骨骼肌微循环;这种影响可能介导有利的结果。然而,目前还没有定义最佳的电流特性。本研究旨在比较使用中高频电流的单次 NMES 治疗对肌肉微循环的影响。
研究了患有全身炎症反应综合征(SIRS)或脓毒症 3-5 天的 ICU 患者和患有 ICUAW 的患者。使用逐渐增加强度的电流对双侧下肢进行 30 分钟的单次 NMES 治疗。患者被随机分配到高频(HF)(75 Hz,脉冲 400 μs,周期 5 秒 ON-21 秒 OFF)或中频(MF)(45 Hz,脉冲 400 μs,周期 5 秒 ON-12 秒 OFF)方案。使用近红外光谱(NIRS)在大鱼际处监测外周微循环,以获得组织氧饱和度(StO2);在治疗前后进行血管闭塞试验。使用 NIRS 还监测了股外侧肌的局部微循环。
31 名患者被随机分配。在 HF 方案(17 名患者)中,外周微循环参数为:鱼际氧消耗率(%/分钟)从 8.6±2.2 增加到 9.9±5.1(P=0.08),内皮反应性(%/秒)从 2.7±1.4 增加到 3.2±1.9(P=0.04),血管储备(秒)从 160±55 减少到 145±49(P=0.03)。在 MF 方案中:鱼际氧消耗率(%/分钟)从 8.8±3.8 增加到 9.9±3.6(P=0.07),内皮反应性(%/秒)从 2.5±1.4 增加到 3.1±1.7(P=0.03),血管储备(秒)从 163±37 减少到 144±33(P=0.001)。两种方案均显示出相似的效果。在股外侧肌中,HF 方案下的平均肌肉氧消耗率为 61±9%/分钟,MF 方案下为 69±23%/分钟(P=0.5)。HF 方案下的 StO2 最小振幅为 5±4 单位,MF 方案下为 7±4 单位(P=0.3)。运动后,HF 方案下的 StO2 增加了 6±7 单位,MF 方案下增加了 5±4 单位(P=0.6)。这些变化与收缩强度密切相关。
单次 NMES 治疗影响局部和全身骨骼肌微循环。中高频电流同样有效。