de Boer Ian H
Corresponding author: Ian H. de Boer,
Diabetes Care. 2014;37(1):24-30. doi: 10.2337/dc13-2113.
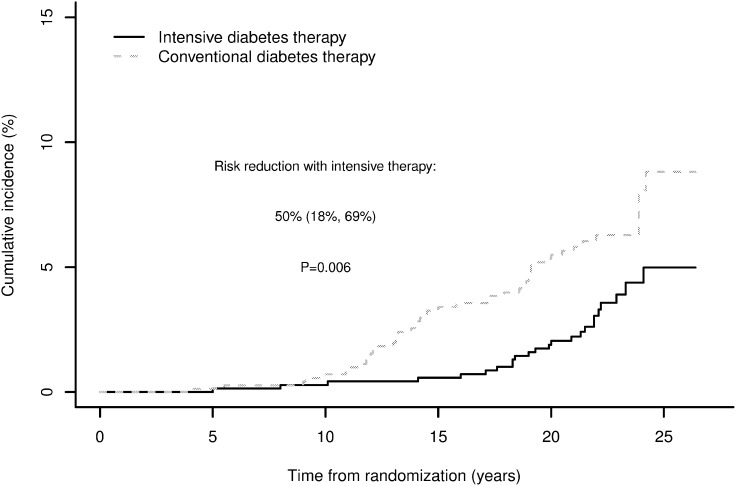
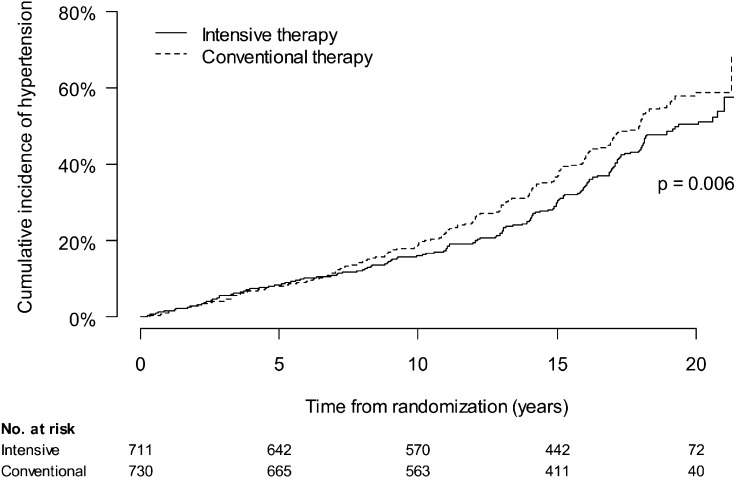
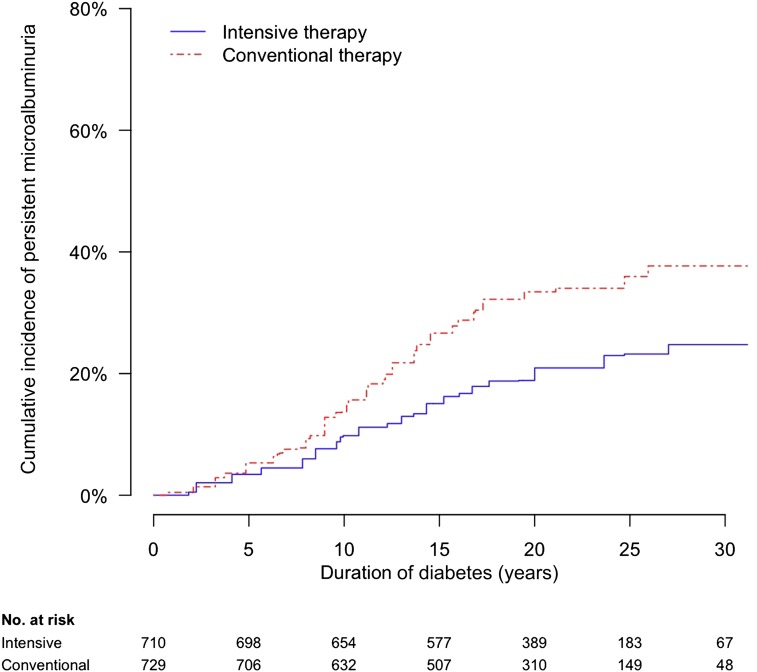
OBJECTIVE Kidney disease manifests clinically as elevated albumin excretion rate (AER), impaired glomerular filtration rate (GFR), or both, and is a cause of substantial morbidity and mortality in type 1 diabetes (T1D). The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) study tested whether intensive diabetes therapy (INT) aimed at lowering glucose concentrations as close as safely possible to the normal range reduces the risks of kidney disease and other diabetes complications. RESEARCH DESIGN AND METHODS In the DCCT, 1,441 participants with T1D were randomly assigned to INT or conventional diabetes therapy (CON) for a mean duration of 6.5 years. Subsequently, participants have been followed for 18 years in the ongoing observational EDIC. Standardized longitudinal measurements of AER, estimated GFR, and blood pressure were made throughout the DCCT/EDIC. RESULTS During the DCCT, INT reduced the risks of incident microalbuminuria (AER ≥40 mg/24 h) and macroalbuminuria (AER ≥300 mg/24 h) by 39% (95% CI 21-52%) and 54% (29-74%), respectively. During EDIC years 1-8, participants previously assigned to DCCT INT continued to experience lower rates of incident microalbuminuria and macroalbuminuria, with risk reductions of 59% (39-73%) and 84% (67-92%), respectively. Beneficial effects of INT on the development of impaired GFR (sustained estimated GFR <60 mL/min/1.73 m(2)) and hypertension became evident during combined DCCT/EDIC follow-up, with risk reductions of 50% (18-69%) and 20% (6-21%), respectively, compared with CON. CONCLUSIONS In the DCCT/EDIC, INT resulted in clinically important, durable reductions in the risks of microalbuminuria, macroalbuminuria, impaired GFR, and hypertension.
目的 肾病在临床上表现为白蛋白排泄率(AER)升高、肾小球滤过率(GFR)受损或两者兼而有之,是1型糖尿病(T1D)患者发病和死亡的重要原因。糖尿病控制与并发症试验/糖尿病干预与并发症流行病学(DCCT/EDIC)研究旨在检验,将血糖浓度尽可能安全地降低至正常范围的强化糖尿病治疗(INT)是否能降低肾病及其他糖尿病并发症的风险。研究设计与方法 在DCCT中,1441例T1D患者被随机分配接受INT或传统糖尿病治疗(CON),平均治疗时间为6.5年。随后,在正在进行的观察性EDIC研究中,对患者进行了18年的随访。在整个DCCT/EDIC期间,对AER、估算的GFR和血压进行了标准化的纵向测量。结果 在DCCT期间,INT使微量白蛋白尿(AER≥40 mg/24 h)和大量白蛋白尿(AER≥300 mg/24 h)的发病风险分别降低了39%(95%CI 21-52%)和54%(29-74%)。在EDIC研究的第1-8年,先前被分配接受DCCT INT治疗的患者,微量白蛋白尿和大量白蛋白尿的发病率仍然较低,风险分别降低了59%(39-73%)和84%(67-92%)。在DCCT/EDIC联合随访期间,INT对GFR受损(估算的GFR持续<60 mL/min/1.73 m²)和高血压发生的有益作用变得明显,与CON组相比,风险分别降低了50%(18-69%)和20%(6-21%)。结论 在DCCT/EDIC研究中,INT显著且持久地降低了微量白蛋白尿、大量白蛋白尿、GFR受损和高血压的风险。