Lichtenstein D
Service de Réanimation Médicale, Hôpital Ambroise-Paré, Université Paris-Ouest, France.
Heart Lung Vessel. 2013;5(3):142-7.
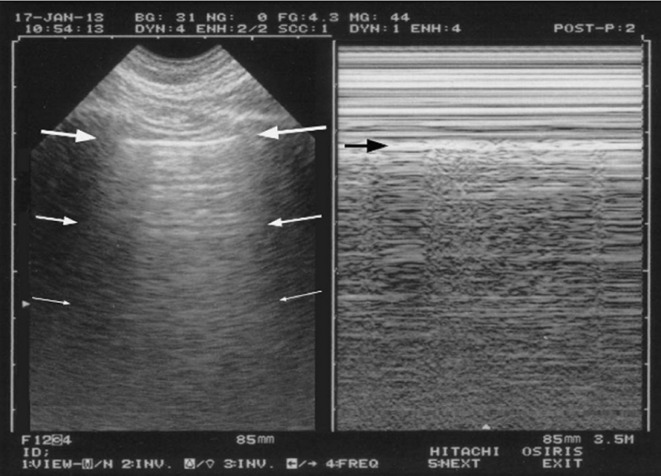
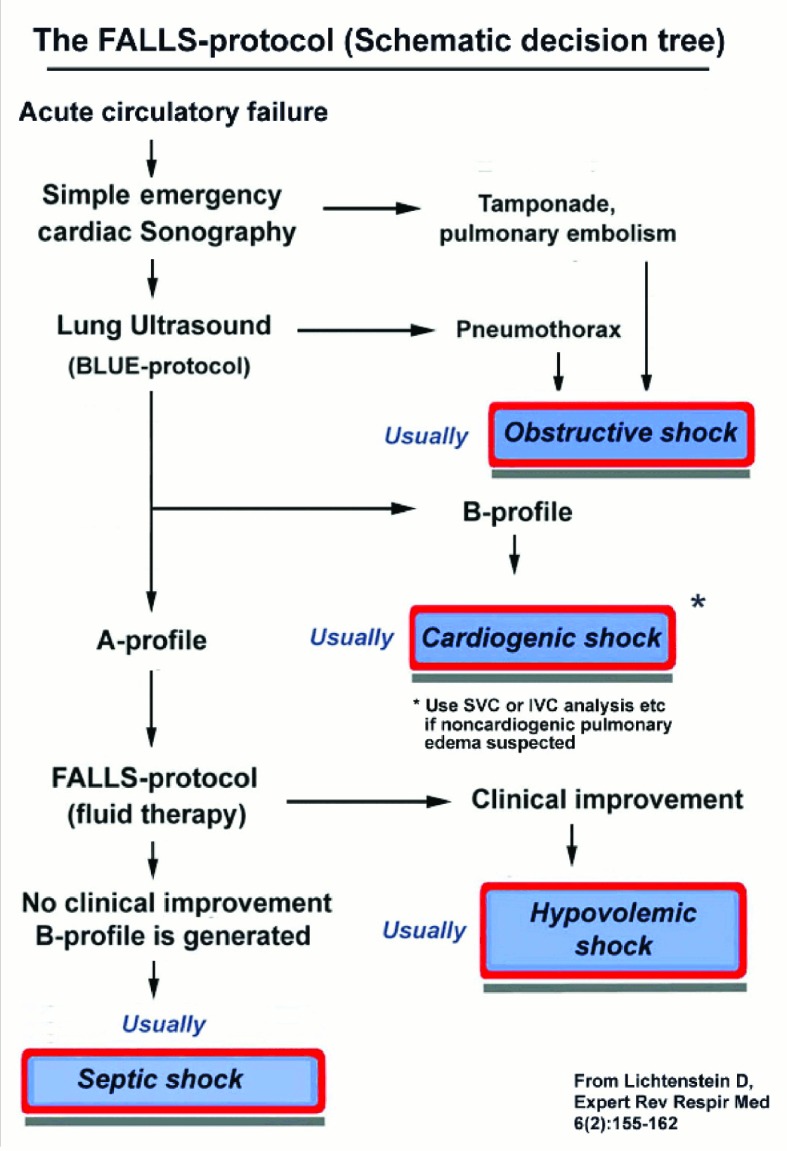
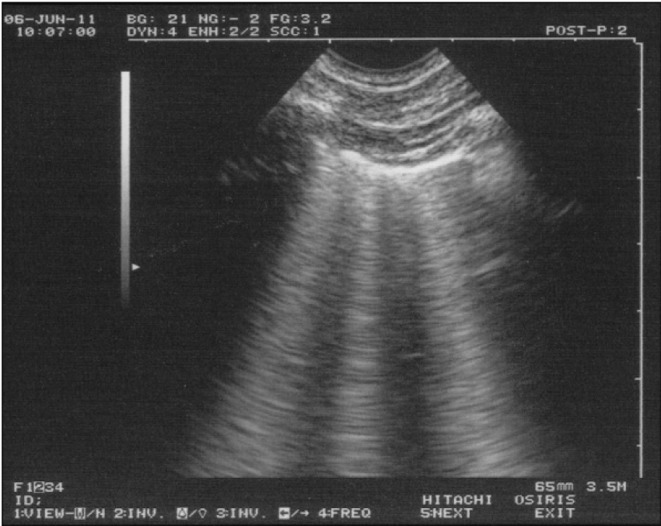
The assessment of acute circulatory failure is a challenge in absence of solid gold standard. It is suggested that artifacts generated by lung ultrasound can be of help. The FALLS-protocol (Fluid Administration Limited by Lung Sonography) follows Weil's classification of shocks. Firstly, it searches for pericardial fluid, then right heart enlargment, lastly abolished lung sliding. In this setting, the diagnoses of pericardial tamponade, pulmonary embolism and tension pneumothorax, i.e. obstructive shock, can be schematically ruled out. Moreover, the search of diffuse lung rockets (i.e. multiple B-lines, a comet-tail artifact) is performed. Its absence excludes pulmonary edema, that in clinical practice is left cardiogenic shock (most cases). At this step, the patient (defined FALLS-responder) receives fluid therapy. He/she has usually a normal sonographic lung surface, an A-profile. Any clinical improvement suggests hypovolemic shock. The absence of improvement generates continuation of fluid therapy, eventually yielding fluid overload. This condition results in the change from A-profile to B-profile. Lung ultrasound has the advantage to demonstrate this interstitial syndrome at an early and infraclinical stage (FALLS-endpoint). The change from horizontal A-lines to vertical B-lines can be considered as a direct marker of volemia in this use. By elimination, this change indicates schematically distributive shock, while in current practice septic shock. The major limitation is the B-profile on admission generated by an initial lung disorder. FALLS-protocol, which can be associated with no drawback with traditional hemodynamic tools, uses a simple machine (without Doppler) and a suitable microconvex probe allowing for heart, lung and vein assessment.
在缺乏可靠金标准的情况下,急性循环衰竭的评估是一项挑战。有人提出,肺部超声产生的伪像可能会有所帮助。FALLS方案(通过肺部超声限制液体输注)遵循韦尔对休克的分类。首先,它寻找心包积液,然后是右心扩大,最后是肺滑动消失。在这种情况下,可以大致排除心包填塞、肺栓塞和张力性气胸,即梗阻性休克的诊断。此外,还要检查是否存在弥漫性肺火箭征(即多条B线,一种彗尾伪像)。其不存在可排除肺水肿,在临床实践中肺水肿通常是心源性休克(大多数情况)。在这一步,患者(定义为FALLS反应者)接受液体治疗。他/她的肺部超声图像通常正常,呈A形。任何临床改善都提示低血容量性休克。无改善则继续进行液体治疗,最终导致液体超负荷。这种情况会导致从A形转变为B形。肺部超声的优势在于能够在早期和亚临床阶段(FALLS终点)显示这种间质综合征。在这种应用中,从水平A线到垂直B线的变化可被视为血容量的直接标志。通过排除法,这种变化大致提示分布性休克,在当前实践中即脓毒性休克。主要局限性在于初始肺部疾病导致入院时出现B形。FALLS方案可与传统血流动力学工具结合使用而无缺点,它使用一台简单的机器(无多普勒)和一个合适的微凸探头,可用于评估心脏、肺部和静脉。