Epicentre, Paris, France.
Instituto Nacional de Saúde, Maputo, Mozambique.
PLoS One. 2013 Dec 18;8(12):e84585. doi: 10.1371/journal.pone.0084585. eCollection 2013.
We used data from a randomized trial of HIV-tuberculosis co-infected patients in Mozambique to determine the incidence and predictors of paradoxical tuberculosis-associated immune reconstitution inflammatory syndrome (IRIS) occurring within 12 weeks of starting antiretroviral therapy, and to evaluate its association with patient outcome at 48 weeks.
HIV-tuberculosis co-infected and antiretroviral therapy-naïve adults with less than 250 CD4/mm3 were randomized to a nevirapine or efavirenz-based antiretroviral therapy initiated 4 to 6 weeks after starting tuberculosis treatment, and were then followed for 48 weeks. Tuberculosis cases were diagnosed using WHO guidelines, and tuberculosis-IRIS by case definitions of the International Network for the Study of HIV-associated IRIS.
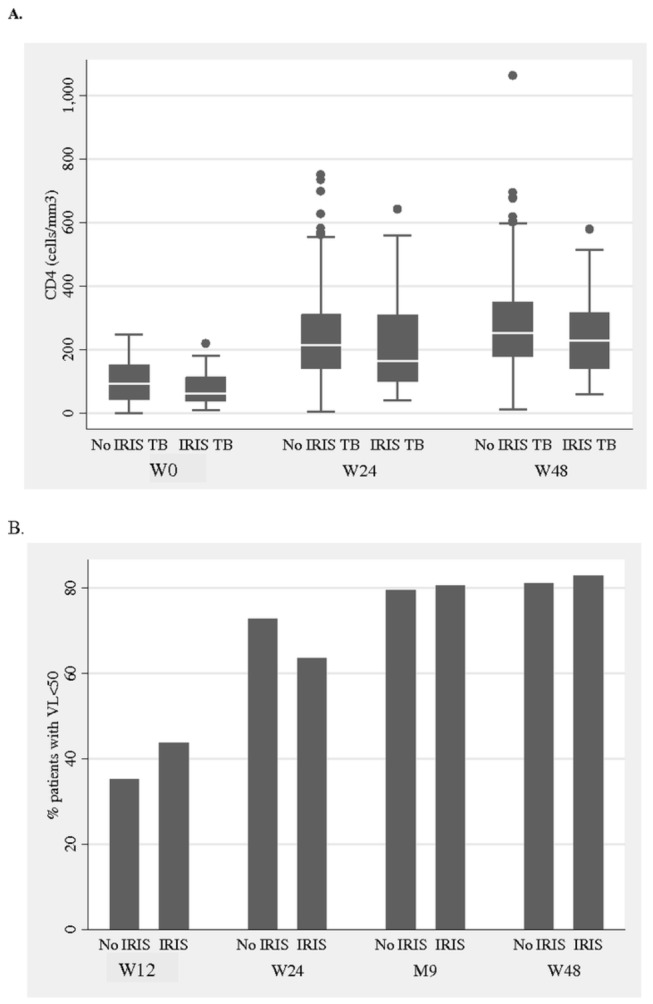
The 573 HIV-tuberculosis co-infected patients who initiated antiretroviral therapy had a median CD4 count of 92 cells/mm(3) and HIV-1 RNA of 5.6 log10 copies/mL. Mortality at week 48 was 6.1% (35/573). Fifty-three (9.2%) patients presented a tuberculosis-IRIS within 12 weeks of starting antiretroviral therapy. Being female and having a low CD4 count, high HIV-1 RNA load, low body mass index and smear-positive pulmonary tuberculosis were independently associated with tuberculosis-IRIS. After adjustment for baseline body mass index, CD4 count and hemoglobin, occurrence of tuberculosis-IRIS was independently associated with 48-week mortality (aOR 2.72 95%CI 1.14-6.54). Immunological and HIV-1 virological responses and tuberculosis treatment outcomes were not different between patients with and without tuberculosis-IRIS.
In this large prospective cohort, tuberculosis-IRIS occurrence within 12 weeks of starting antiretroviral therapy was independently associated with the mortality of HIV-tuberculosis co-infected patients at 48 weeks post antiretroviral therapy initiation.
我们使用莫桑比克艾滋病毒-结核分枝杆菌合并感染患者的随机试验数据,确定在开始抗逆转录病毒治疗后 12 周内发生的结核相关免疫重建炎症综合征(IRIS)的发生率和预测因素,并评估其与 48 周时患者结局的关系。
HIV-结核分枝杆菌合并感染且未接受过抗逆转录病毒治疗、CD4 细胞计数<250 个/mm3 的成年人在开始结核病治疗后 4 至 6 周内随机接受基于奈韦拉平或依非韦伦的抗逆转录病毒治疗,并随后随访 48 周。结核病病例采用世界卫生组织指南诊断,结核 IRIS 采用 HIV 相关 IRIS 国际网络的病例定义。
573 名开始抗逆转录病毒治疗的 HIV-结核分枝杆菌合并感染患者的中位 CD4 计数为 92 个细胞/mm3,HIV-1 RNA 为 5.6log10 拷贝/mL。48 周时的死亡率为 6.1%(35/573)。53 例(9.2%)患者在开始抗逆转录病毒治疗后 12 周内出现结核 IRIS。女性、CD4 计数低、HIV-1 RNA 载量高、低体重指数和痰涂片阳性肺结核是与结核 IRIS 独立相关的因素。在调整基线体重指数、CD4 计数和血红蛋白后,发生结核 IRIS 与 48 周死亡率独立相关(调整后比值比 2.72,95%CI 1.14-6.54)。结核 IRIS 患者与无结核 IRIS 患者的免疫和 HIV-1 病毒学反应及结核病治疗结局无差异。
在这项大型前瞻性队列研究中,开始抗逆转录病毒治疗后 12 周内发生结核 IRIS 与开始抗逆转录病毒治疗后 48 周时 HIV-结核分枝杆菌合并感染患者的死亡率独立相关。