Donahue Timothy F, Bochner Bernard H, Sfakianos John P, Kent Matthew, Bernstein Melanie, Hilton William M, Cha Eugene K, Yee Alyssa M, Dalbagni Guido, Vargas Hebert A
Urology Service, Department of Surgery, Memorial Sloan-Kettering Cancer Center, New York, New York.
Department of Epidemiology and Biostatistics, Memorial Sloan-Kettering Cancer Center, New York, New York.
J Urol. 2014 Jun;191(6):1708-13. doi: 10.1016/j.juro.2013.12.041. Epub 2013 Dec 30.
Parastomal hernia is a frequent complication of stoma formation after radical cystectomy. We determined the prevalence and risk factors for the development of parastomal hernia after radical cystectomy.
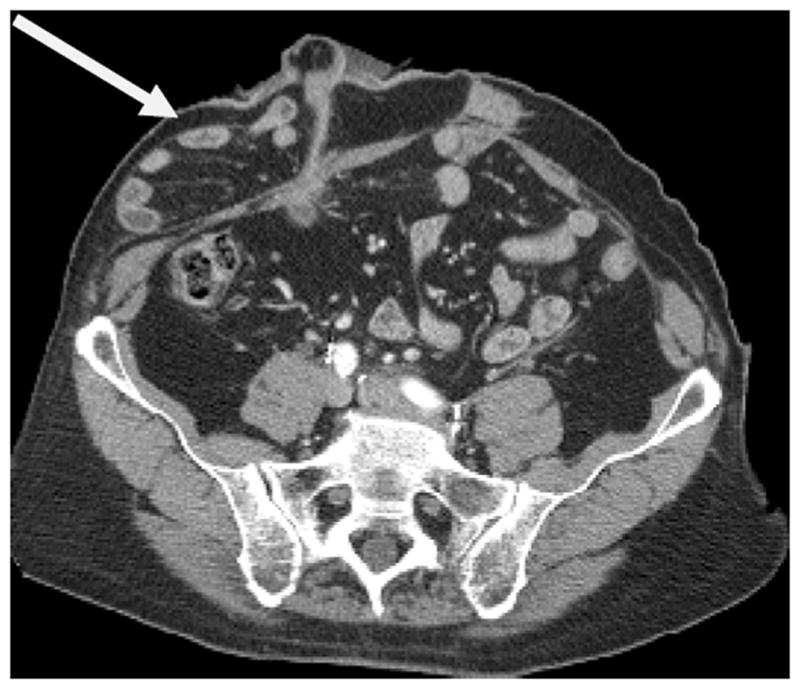
We conducted a retrospective study of 433 consecutive patients who underwent open radical cystectomy and ileal conduit between 2006 and 2010. Postoperative cross-sectional imaging studies performed for routine oncologic followup (1,736) were evaluated for parastomal hernia, defined as radiographic evidence of protrusion of abdominal contents through the abdominal wall defect created by forming the stoma. Univariable and multivariable Cox regression analyses were used to determine clinical and surgical factors associated with parastomal hernia.
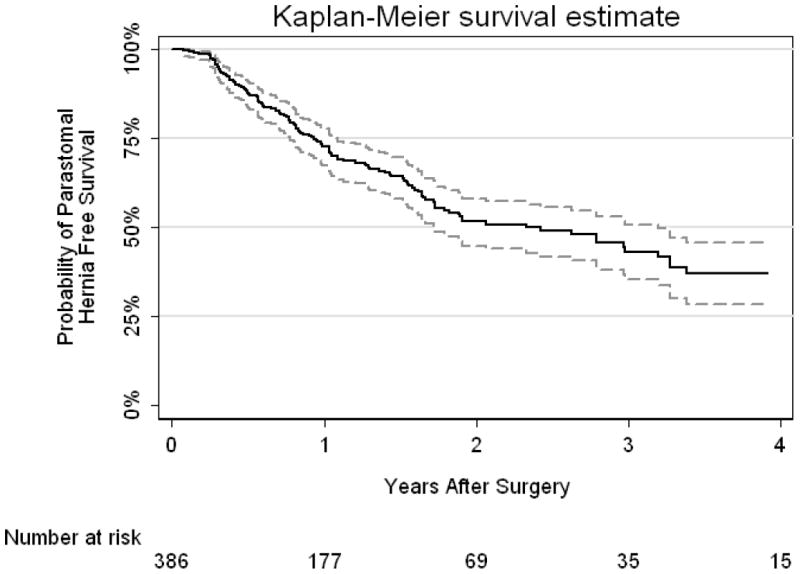
Complete data were available for 386 patients with radiographic parastomal hernia occurring in 136. The risk of a parastomal hernia developing was 27% (95% CI 22, 33) and 48% (95% CI 42, 55) at 1 and 2 years, respectively. Clinical diagnosis of parastomal hernia was documented in 93 patients and 37 were symptomatic. Of 16 patients with clinical parastomal hernia referred for repair 8 had surgery. On multivariable analysis female gender (HR 2.25; 95% CI 1.58, 3.21; p<0.0001), higher body mass index (HR 1.08 per unit increase; 95% CI 1.05, 1.12; p<0.0001) and lower preoperative albumin (HR 0.43 per gm/dl; 95% CI 0.25, 0.75; p=0.003) were significantly associated with parastomal hernia.
The overall risk of radiographic evidence of parastomal hernia approached 50% at 2 years. Female gender, higher body mass index and lower preoperative albumin were most associated with the development of parastomal hernia. Identifying those at greatest risk may allow for prospective surgical maneuvers at the time of initial surgery, such as placement of prophylactic mesh in selected patients, to prevent the occurrence of parastomal hernia.
造口旁疝是根治性膀胱切除术后造口形成常见的并发症。我们确定了根治性膀胱切除术后造口旁疝发生的患病率及危险因素。
我们对2006年至2010年间连续433例行开放性根治性膀胱切除术及回肠代膀胱术的患者进行了一项回顾性研究。对为进行常规肿瘤学随访而进行的术后横断面影像学检查(共1736次)进行评估,以确定造口旁疝,造口旁疝定义为通过造口形成的腹壁缺损有腹部内容物突出的影像学证据。采用单变量和多变量Cox回归分析来确定与造口旁疝相关的临床和手术因素。
386例患者有完整数据,其中136例出现影像学造口旁疝。造口旁疝发生风险在1年和2年时分别为27%(95%可信区间22, 33)和48%(95%可信区间42, 55)。93例患者有造口旁疝的临床诊断记录,其中37例有症状。在16例因临床造口旁疝转诊进行修复的患者中,8例接受了手术。多变量分析显示,女性(风险比2.25;95%可信区间1.58, 3.21;p<0.0001)、较高的体重指数(每增加一个单位风险比1.08;95%可信区间1.05, 1.12;p<0.0001)和较低的术前白蛋白水平(每克/分升风险比0.43;95%可信区间0.25, )与造口旁疝显著相关。
2年时出现造口旁疝影像学证据的总体风险接近50%。女性、较高的体重指数和较低的术前白蛋白水平与造口旁疝的发生最为相关。识别出风险最高的患者,可能有助于在初次手术时采取前瞻性手术操作,如在部分患者中放置预防性补片,以预防造口旁疝的发生。