Dhermain Frederic
Department of Radiation Oncology, Institut Gustave Roussy University Hospital, Villejuif 94805, France.
Chin J Cancer. 2014 Jan;33(1):16-24. doi: 10.5732/cjc.013.10217.
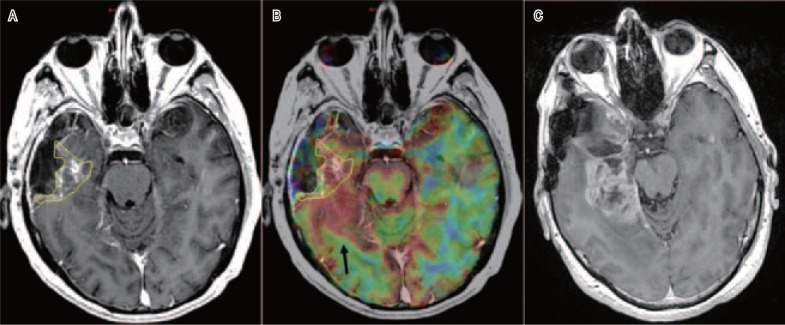
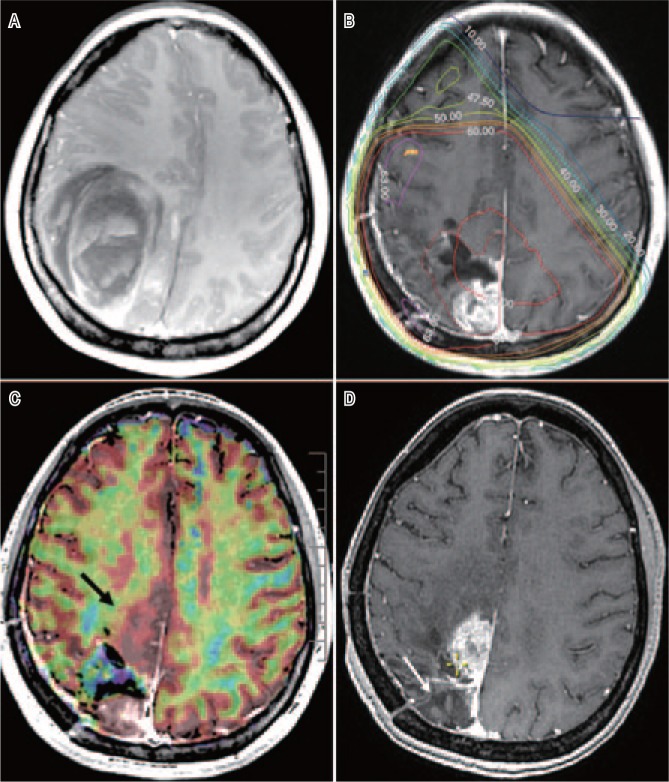
The current standards in radiotherapy of high-grade gliomas (HGG) are based on anatomic imaging techniques, usually computed tomography (CT) scanning and magnetic resonance imaging (MRI). The guidelines vary depending on whether the HGG is a histological grade 3 anaplastic glioma (AG) or a grade 4 glioblastoma multiforme (GBM). For AG, T2-weighted MRI sequences plus the region of contrast enhancement in T1 are considered for the delineation of the gross tumor volume (GTV), and an isotropic expansion of 15 to 20 mm is recommended for the clinical target volume (CTV). For GBM, the Radiation Therapy Oncology Group favors a two-step technique, with an initial phase (CTV1) including any T2 hyperintensity area (edema) plus a 20 mm margin treated with up to 46 Gy in 23 fractions, followed by a reduction in CTV2 to the contrast enhancement region in T1 with an additional 25 mm margin. The European Organisation of Research and Treatment of Cancer recommends a single-phase technique with a unique GTV, which comprises the T1 contrast enhancement region plus a margin of 20 to 30 mm. A total dose of 60 Gy in 30 fractions is usually delivered for GBM, and a dose of 59.4 Gy in 33 fractions is typically given for AG. As more than 85% of HGGs recur in field, dose-escalation studies have shown that 70 to 75 Gy can be delivered in 6 weeks with relevant toxicities developing in <10% of the patients. However, the only randomized dose-escalation trial, in which the boost dose was guided by conventional MRI, did not show any survival advantage of this treatment over the reference arm. HGGs are amongst the most infiltrative and heterogeneous tumors, and it was hypothesized that the most highly aggressive areas were missed; thus, better visualization of these high-risk regions for radiation boost could decrease the recurrence rate. Innovations in imaging and linear accelerators (LINAC) could help deliver the right doses of radiation to the right subvolumes according to the dose-painting concept. Advanced imaging techniques provide functional information on cellular density (diffusion MRI), angiogenesis (perfusion MRI), metabolic activity and cellular proliferation [positron emission tomography (PET) and magnetic resonance spectroscopy (MRS)]. All of these non-invasive techniques demonstrated good association between the images and histology, with up to 40% of HGGs functionally presenting a high activity within the non-contrast-enhanced areas in T1. New LINAC technologies, such as intensity-modulated and stereotactic radiotherapy, help to deliver a simultaneous integrated boost (SIB) > 60 Gy. Trials delivering a SIB into a biological GTV showed the feasibility of this treatment, but the final results, in terms of clinical benefits for HGG patients, are still pending. Many issues have been identified: the variety of MRI and PET machines (and amino-acid tracers), the heterogeneity of the protocols used for image acquisition and post-treatment, the geometric distortion and the unreliable algorithms for co-registration of brain anatomy with functional maps, and the semi-quiescent but highly invasive HGG cells. These issues could be solved by the homogenization of the protocols and software applications, the simultaneous acquisition of anatomic and functional images (PET-MRI machines), the combination of complementary imaging tools (perfusion and diffusion MRI), and the concomitant addition of some ad hoc targeted drugs against angiogenesis and invasiveness to chemoradiotherapy. The integration of these hybrid data will construct new synthetic metrics for fully individualized treatments.
高级别胶质瘤(HGG)放疗的当前标准基于解剖成像技术,通常是计算机断层扫描(CT)和磁共振成像(MRI)。指南因HGG是组织学3级间变性胶质瘤(AG)还是4级多形性胶质母细胞瘤(GBM)而异。对于AG,T2加权MRI序列加上T1加权成像中的对比增强区域用于勾勒大体肿瘤体积(GTV),建议临床靶体积(CTV)进行各向同性扩展15至20毫米。对于GBM,放射治疗肿瘤学组倾向于采用两步技术,初始阶段(CTV1)包括任何T2高信号区域(水肿)加上20毫米边缘,分23次给予高达46 Gy的剂量,随后将CTV2缩小至T1加权成像中的对比增强区域,并额外增加25毫米边缘。欧洲癌症研究与治疗组织推荐采用单相技术,即单一GTV,其包括T1加权成像对比增强区域加上20至30毫米的边缘。GBM通常分30次给予60 Gy的总剂量,AG通常分33次给予59.4 Gy的剂量。由于超过85%的HGG在野内复发,剂量递增研究表明,6周内可给予70至75 Gy的剂量,<10%的患者会出现相关毒性。然而,唯一一项随机剂量递增试验,其推量剂量由传统MRI引导,并未显示该治疗相对于对照臂有任何生存优势。HGG是最具浸润性和异质性的肿瘤之一,据推测最具侵袭性的区域被遗漏了;因此,更好地显示这些用于放射推量的高风险区域可能会降低复发率。成像和直线加速器(LINAC)的创新有助于根据剂量描绘概念将正确剂量的辐射传递到正确的子体积。先进的成像技术可提供有关细胞密度(扩散MRI)、血管生成(灌注MRI)、代谢活性和细胞增殖的功能信息[正电子发射断层扫描(PET)和磁共振波谱(MRS)]。所有这些非侵入性技术都显示出图像与组织学之间有良好的相关性,高达40%的HGG在T1加权成像的非对比增强区域内功能上呈现高活性。新的LINAC技术,如调强放疗和立体定向放疗,有助于给予同步整合推量(SIB)>60 Gy。将SIB应用于生物学GTV的试验表明了这种治疗的可行性,但就HGG患者的临床益处而言,最终结果仍有待确定。已发现许多问题:MRI和PET机器(以及氨基酸示踪剂)的多样性、用于图像采集和治疗后处理的方案的异质性、几何畸变以及用于脑解剖结构与功能图谱配准的不可靠算法,以及半静止但高度侵袭性的HGG细胞。这些问题可以通过使方案和软件应用同质化、同时采集解剖和功能图像(PET-MRI机器)、结合互补成像工具(灌注和扩散MRI)以及在放化疗中同时添加一些针对血管生成和侵袭性的特殊靶向药物来解决。这些混合数据的整合将构建用于完全个体化治疗的新综合指标。