Miyatake Shin-Ichi, Kawabata Shinji, Hiramatsu Ryo, Furuse Motomasa, Kuroiwa Toshihiko, Suzuki Minoru
Department of Neurosurgery, Osaka Medical College, Osaka, Japan.
Radiat Oncol. 2014 Jan 6;9:6. doi: 10.1186/1748-717X-9-6.
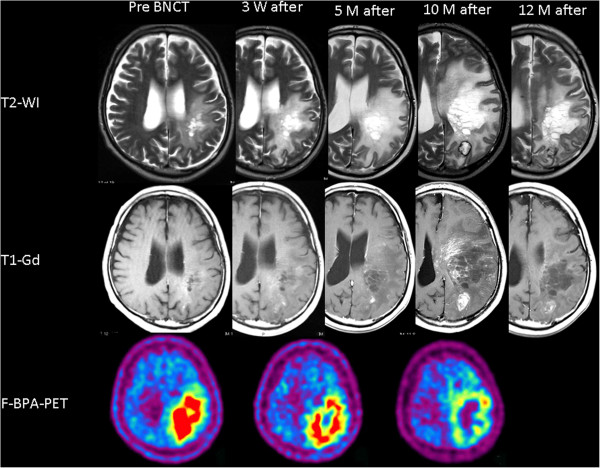
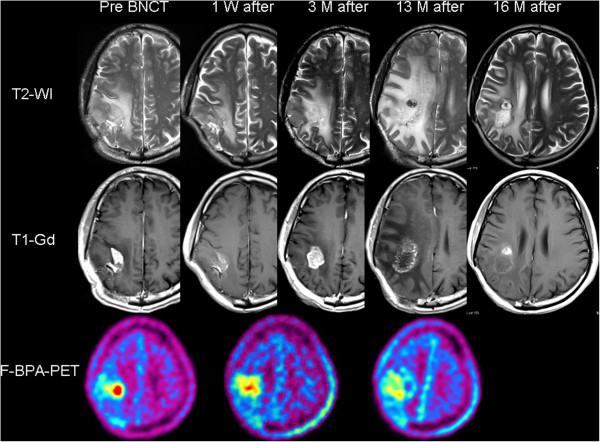
Recurrent malignant gliomas (RMGs) are very difficult to control, and no standard treatments have been established for them. We performed boron neutron capture therapy (BNCT) for patients with RMG. BNCT enables high-dose particle radiation to be applied selectively to tumor cells. However, RMG cases generally receive nearly 60 Gy X-ray irradiation prior to re-irradiation by BNCT. Therefore, even with tumor-selective particle radiation BNCT, radiation necrosis in the brain and symptomatic pseudoprogression may develop. In four of our recent patients with RMG after BNCT, we applied the anti-VEGF antibody bevacizumab to treat two pathological entities. This approach appeared to prolong survival. Here we present the case reports of these four consecutive patients with RMG and discuss the novel use of bevacizumab in this context.
Four patients with RMGs were treated with BNCT at our institutes. Upon the referral for BNCT, they were assessed as belonging to the recursive partitioning analysis (RPA) class 3 (n = 3 patients) or RPA class 4 (n = 1 patient) (the RPA classification for RMG was advocated by Carson et al. in 2007). The estimated median survival times for RPA classes 3 and 4 were 3.8 and 10.8 months, respectively, after some treatment at the recurrence. We applied BNCT for these four patients and administered bevacizumab when the lesions were considered radiation necrosis or symptomatic pseudoprogression. The class 3 patients survived after the BNCT for 14, 16.5 and > 23 months, and the class 4 patient survived > 26 months, with favorable improvements in clinical symptoms.
BNCT with the addition of bevacizumab for radiation necrosis or symptomatic pseudoprogression improved the clinical symptoms and prolonged the survival in RMG patients.
复发性恶性胶质瘤(RMG)极难控制,目前尚未确立针对其的标准治疗方法。我们对RMG患者进行了硼中子俘获疗法(BNCT)。BNCT能够将高剂量粒子辐射选择性地作用于肿瘤细胞。然而,RMG病例在接受BNCT再照射之前通常已接受近60 Gy的X射线照射。因此,即使采用肿瘤选择性粒子辐射的BNCT,仍可能发生脑内放射性坏死和症状性假性进展。在我们最近的4例接受BNCT治疗后的RMG患者中,我们应用抗血管内皮生长因子(VEGF)抗体贝伐单抗治疗两种病理情况。这种方法似乎延长了生存期。在此,我们展示这4例连续的RMG患者的病例报告,并讨论贝伐单抗在此情况下的新用途。
4例RMG患者在我们的机构接受了BNCT治疗。在转诊接受BNCT时,他们被评估为属于递归分区分析(RPA)3级(n = 3例患者)或RPA 4级(n = 1例患者)(RMG的RPA分类由Carson等人于2007年提出)。复发后经过一些治疗,RPA 3级和4级的估计中位生存期分别为3.8个月和10.8个月。我们对这4例患者进行了BNCT,并在病变被认为是放射性坏死或症状性假性进展时给予贝伐单抗。3级患者在BNCT后存活了14、16.5和> 23个月,4级患者存活> 26个月,临床症状有良好改善。
BNCT联合贝伐单抗治疗放射性坏死或症状性假性进展改善了RMG患者的临床症状并延长了生存期。