1] Section of Gastroenterology, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire, USA [2] Department of Medicine, Geisel School of Medicine at Dartmouth, Hanover, New Hampshire, USA.
Department of Community and Family Medicine, Geisel School of Medicine at Dartmouth, Hanover, New Hampshire, USA.
Am J Gastroenterol. 2014 Mar;109(3):417-26. doi: 10.1038/ajg.2013.442. Epub 2014 Jan 7.
Detection and removal of adenomas and clinically significant serrated polyps (CSSPs) is critical to the effectiveness of colonoscopy in preventing colorectal cancer. Although longer withdrawal time has been found to increase polyp detection, this association and the use of withdrawal time as a quality indicator remains controversial. Few studies have reported on withdrawal time and serrated polyp detection. Using data from the New Hampshire Colonoscopy Registry, we examined how an endoscopist's withdrawal time in normal colonoscopies affects adenoma and serrated polyp detection.
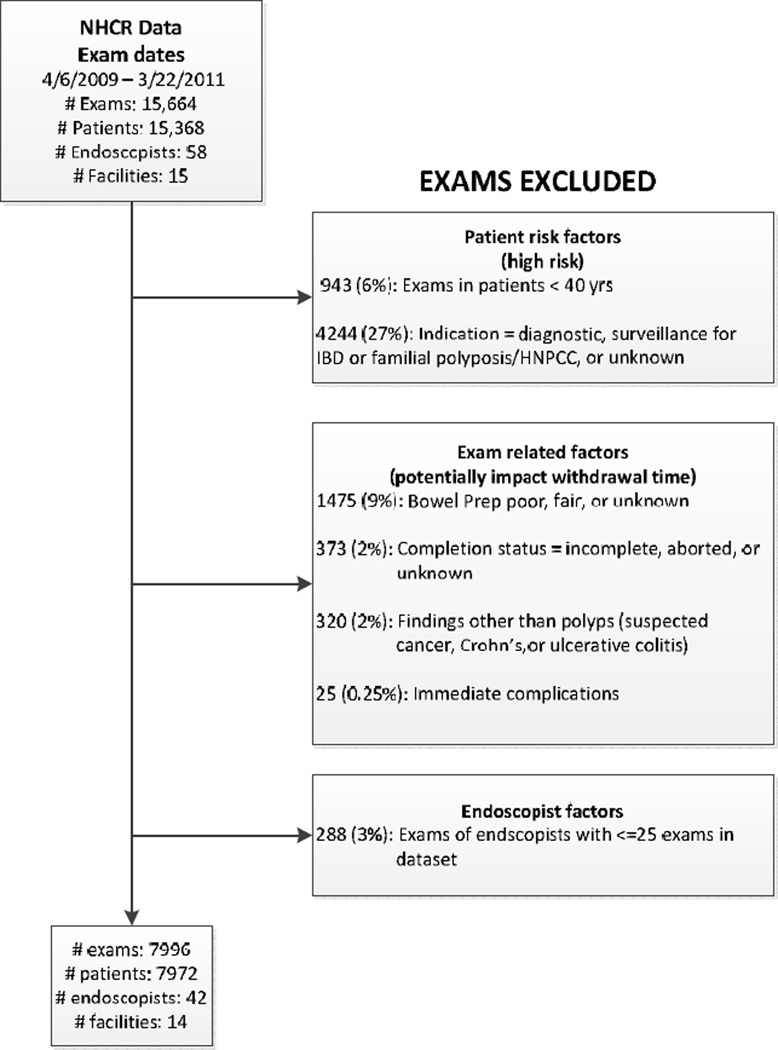
We analyzed 7,996 colonoscopies performed in 7,972 patients between 2009 and 2011 by 42 endoscopists at 14 hospitals, ambulatory surgery centers, and community practices. CSSPs were defined as sessile serrated polyps and hyperplastic polyps proximal to the sigmoid. Adenoma and CSSP detection rates were calculated based on median endoscopist withdrawal time in normal exams. Regression models were used to estimate the association of increased normal withdrawal time and polyp, adenoma, and CSSP detection.
Polyp and adenoma detection rates were highest among endoscopists with 9 min median normal withdrawal time, and detection of CSSPs reached its highest levels at 8-9 min. Incident rate ratios for adenoma and CSSP detection increased with each minute of normal withdrawal time above 6 min, with maximum benefit at 9 min for adenomas (1.50, 95% confidence interval (CI) (1.21, 1.85)) and CSSPs (1.77, 95% CI (1.15, 2.72)). When modeling was used to set the minimum withdrawal time at 9 min, we predicted that adenomas and CSSPs would be detected in 302 (3.8%) and 191 (2.4%) more patients. The increase in detection was most striking for the CSSPs, with nearly a 30% relative increase.
A withdrawal time of 9 min resulted in a statistically significant increase in adenoma and serrated polyp detection. Colonoscopy quality may improve with a median normal withdrawal time benchmark of 9 min.
腺瘤和临床上显著锯齿状息肉(CSSP)的检测和切除对于结肠镜检查预防结直肠癌的有效性至关重要。虽然已经发现延长退出时间可以增加息肉的检出率,但这种关联以及将退出时间作为质量指标的使用仍然存在争议。很少有研究报告退出时间和锯齿状息肉的检出率。利用新罕布什尔州结肠镜检查登记处的数据,我们研究了正常结肠镜检查中内镜医师的退出时间如何影响腺瘤和锯齿状息肉的检出率。
我们分析了 2009 年至 2011 年间由 14 家医院、门诊手术中心和社区诊所的 42 名内镜医师对 7972 名患者进行的 7996 例结肠镜检查。CSSP 定义为无蒂锯齿状息肉和乙状结肠近端增生性息肉。根据正常检查中内镜医师的中位退出时间计算腺瘤和 CSSP 的检出率。回归模型用于估计增加正常退出时间与息肉、腺瘤和 CSSP 检出的关联。
在退出时间中位数为 9 分钟的内镜医师中,息肉和腺瘤的检出率最高,而 CSSP 的检出率在 8-9 分钟时达到最高水平。与退出时间中位数超过 6 分钟时每分钟相比,腺瘤和 CSSP 检出率的发生率比值均增加,9 分钟时最大获益(腺瘤 1.50,95%置信区间(CI)(1.21,1.85);CSSP 1.77,95%CI(1.15,2.72))。当使用模型将最低退出时间设定为 9 分钟时,我们预测会有 302(3.8%)和 191(2.4%)例更多的患者检出腺瘤和 CSSP。CSSP 的检出率增加最为显著,相对增加近 30%。
退出时间为 9 分钟可显著增加腺瘤和锯齿状息肉的检出率。以 9 分钟的中位数正常退出时间为基准,结肠镜检查质量可能会提高。