Wolpin S E, Halpenny B, Whitman G, McReynolds J, Stewart M, Lober W B, Berry D L
University of Washington, USA
Dana-Farber Cancer Institute, USA.
Health Informatics J. 2015 Mar;21(1):10-23. doi: 10.1177/1460458213495744. Epub 2014 Jan 9.
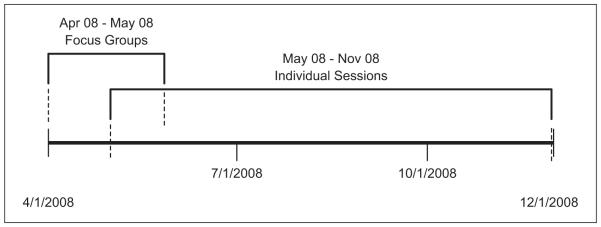
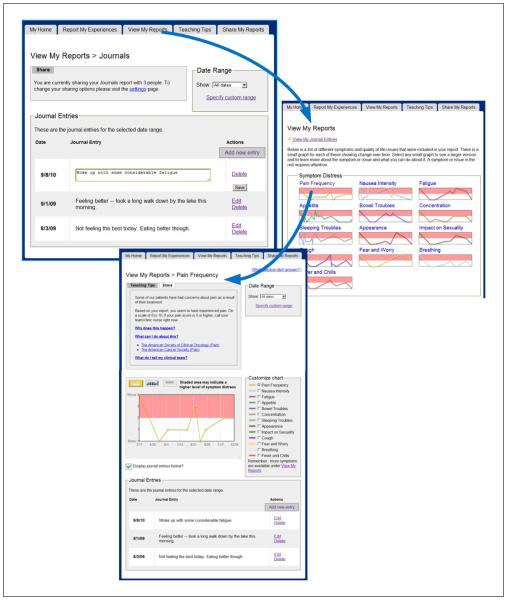
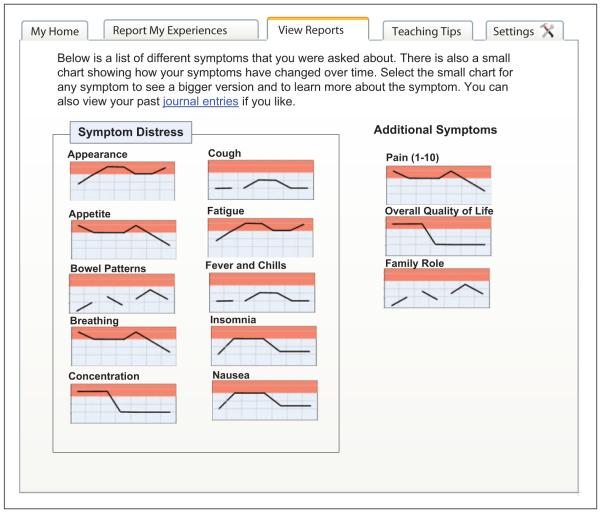
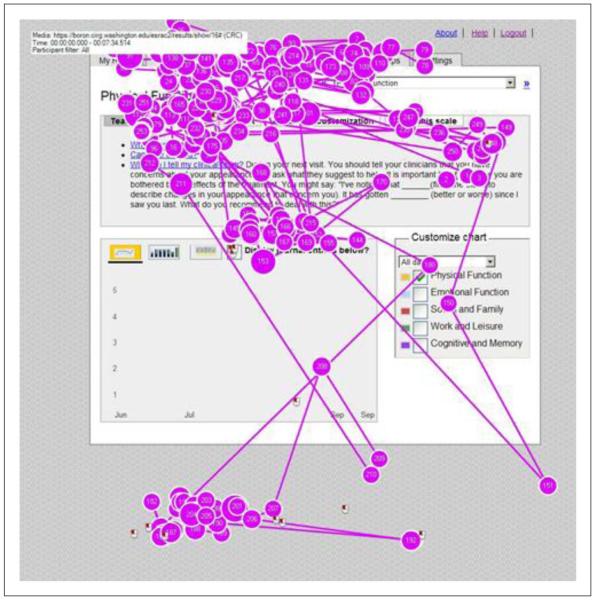
The feasibility and acceptability of computerized screening and patient-reported outcome measures have been demonstrated in the literature. However, patient-centered management of health information entails two challenges: gathering and presenting data using "patient-tailored" methods and supporting "patient-control" of health information. The design and development of many symptom and quality-of-life information systems have not included opportunities for systematically collecting and analyzing user input. As part of a larger clinical trial, the Electronic Self-Report Assessment for Cancer-II project, participatory design approaches were used to build and test new features and interfaces for patient/caregiver users. The research questions centered on patient/caregiver preferences with regard to the following: (a) content, (b) user interface needs, (c) patient-oriented summary, and (d) patient-controlled sharing of information with family, caregivers, and clinicians. Mixed methods were used with an emphasis on qualitative approaches; focus groups and individual usability tests were the primary research methods. Focus group data were content analyzed, while individual usability sessions were assessed with both qualitative and quantitative methods. We identified 12 key patient/caregiver preferences through focus groups with 6 participants. We implemented seven of these preferences during the iterative design process. We deferred development for some of the preferences due to resource constraints. During individual usability testing (n = 8), we were able to identify 65 usability issues ranging from minor user confusion to critical errors that blocked task completion. The participatory development model that we used led to features and design revisions that were patient centered. We are currently evaluating new approaches for the application interface and for future research pathways. We encourage other researchers to adopt user-centered design approaches when building patient-centered technologies.
计算机化筛查和患者报告结局测量的可行性和可接受性已在文献中得到证实。然而,以患者为中心的健康信息管理面临两个挑战:使用“患者定制”方法收集和呈现数据,以及支持患者对健康信息的“控制”。许多症状和生活质量信息系统的设计和开发并未包含系统收集和分析用户输入的机会。作为一项更大规模临床试验(癌症电子自我报告评估-II项目)的一部分,采用参与式设计方法为患者/护理人员用户构建和测试新功能及界面。研究问题集中在患者/护理人员对以下方面的偏好:(a) 内容,(b) 用户界面需求,(c) 以患者为导向的总结,以及 (d) 与家人、护理人员和临床医生进行患者控制的信息共享。采用了混合方法,重点是定性方法;焦点小组和个体可用性测试是主要研究方法。对焦点小组数据进行了内容分析,而个体可用性测试则采用定性和定量方法进行评估。通过与6名参与者进行焦点小组讨论,我们确定了12项关键的患者/护理人员偏好。在迭代设计过程中,我们实施了其中7项偏好。由于资源限制,我们推迟了部分偏好的开发。在个体可用性测试(n = 8)期间,我们能够识别出65个可用性问题,范围从轻微的用户困惑到阻碍任务完成的严重错误。我们使用的参与式开发模型带来了以患者为中心的功能和设计修订。我们目前正在评估应用界面的新方法以及未来的研究途径。我们鼓励其他研究人员在构建以患者为中心的技术时采用以用户为中心的设计方法。