Cornec Divi, Saraux Alain, Pers Jacques-Olivier, Jousse-Joulin Sandrine, Marhadour Thierry, Roguedas-Contios Anne-Marie, Genestet Steeve, Renaudineau Yves, Devauchelle-Pensec Valérie
Arthritis Res Ther. 2014 Jan 17;16(1):R15. doi: 10.1186/ar4442.
The aims of this study were to evaluate the diagnostic accuracy of blood B-cell subset profiling and immune-system activation marker assays in primary Sjögren's syndrome (pSS) and to assess whether adding these tools to the current laboratory item would improve the American-European Consensus Group (AECG) criteria.
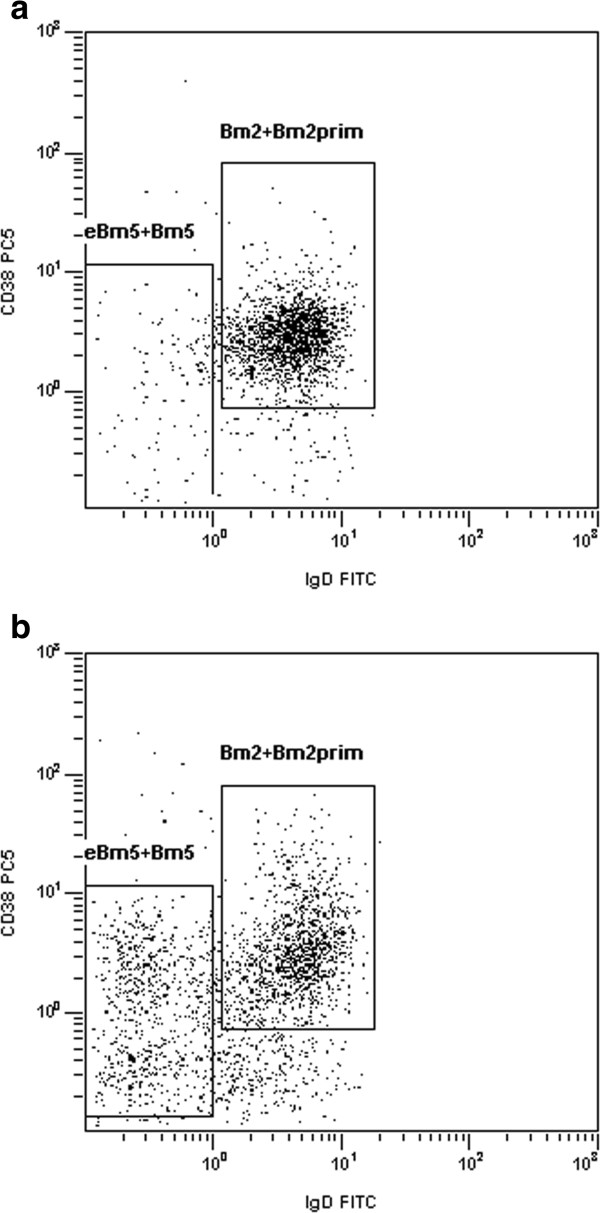
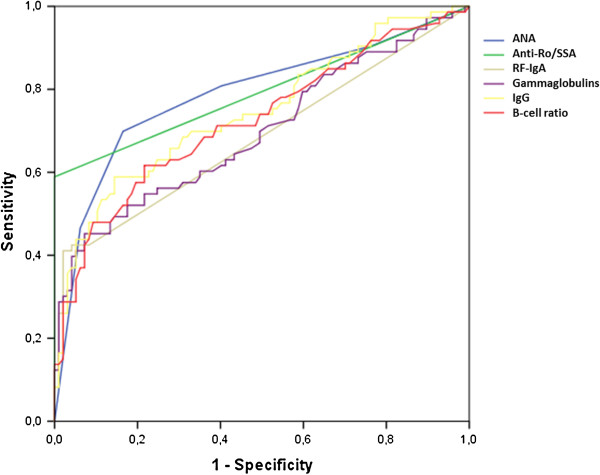
In a single-center cohort of patients with suspected pSS, we tested the diagnostic performance of anti-SSA, antinuclear antibody (ANA), rheumatoid factor (RF), gammaglobulins, IgG titers, and B-cell ratio defined as (Bm2 + Bm2')/(eBm5 + Bm5), determined using flow cytometry. The reference standard was a clinical diagnosis of pSS established by a panel of experts.
Of 181 patients included in the study, 77 had pSS. By logistic regression analysis, only ANA ≥1:640 (sensitivity, 70.4%; specificity 83.2%) and B-cell ratio ≥5 (sensitivity, 52.1%; specificity, 83.2%) showed independent associations with pSS of similar strength. In anti-SSA-negative patients, presence of either of these two criteria had 71.0% sensitivity but only 67.3% specificity for pSS; whereas combining both criteria had 96.2% specificity but only 12.9% sensitivity. Adding either of these two criteria to the AECG criteria set increased sensitivity from 83.1% to 90.9% but decreased specificity from 97.1% to 85.6%, whereas adding both criteria in combination did not substantially modify the diagnostic performance of the criteria set. The adjunction of RF + ANA ≥1:320, as proposed in the new American College of Rheumatology (ACR) criteria, did not improve the diagnostic value of anti-SSA.
Blood B-cell subset profiling is a simple test that has good diagnostic properties for pSS. However, adding this test, with or without ANA positivity, does not improve current classification criteria.
本研究旨在评估血液B细胞亚群分析和免疫系统激活标志物检测在原发性干燥综合征(pSS)中的诊断准确性,并评估将这些检测方法添加到当前实验室项目中是否会改善欧美共识小组(AECG)标准。
在一个单中心疑似pSS患者队列中,我们检测了抗SSA、抗核抗体(ANA)、类风湿因子(RF)、γ球蛋白、IgG滴度以及通过流式细胞术测定的定义为(Bm2 + Bm2')/(eBm5 + Bm5)的B细胞比例的诊断性能。参考标准是由一组专家确立的pSS临床诊断。
在纳入研究的181例患者中,77例患有pSS。通过逻辑回归分析,只有ANA≥1:640(敏感性70.4%;特异性83.2%)和B细胞比例≥5(敏感性52.1%;特异性83.2%)显示出与pSS具有相似强度的独立关联。在抗SSA阴性患者中,这两个标准中的任何一个对于pSS的敏感性为71.0%,但特异性仅为67.3%;而将两个标准结合使用时,特异性为96.2%,但敏感性仅为12.9%。将这两个标准中的任何一个添加到AECG标准集中可使敏感性从83.1%提高到90.9%,但特异性从97.1%降低到85.6%,而同时添加两个标准并未实质性改变标准集的诊断性能。如新美国风湿病学会(ACR)标准所提议的,添加RF + ANA≥1:320并未提高抗SSA的诊断价值。
血液B细胞亚群分析是一项简单的检测,对pSS具有良好的诊断特性。然而,添加此项检测,无论ANA是否阳性,均不能改善当前的分类标准。