Jones J M, Skaga N O, Søvik S, Lossius H M, Eken T
Mathematics Department, Keele University, Keele, Staffordshire, United Kingdom.
Acta Anaesthesiol Scand. 2014 Mar;58(3):303-15. doi: 10.1111/aas.12256. Epub 2014 Jan 20.
Anatomic injury, physiological derangement, age, and injury mechanism are well-founded predictors of trauma outcome. We aimed to develop and validate the first Scandinavian survival prediction model for trauma.
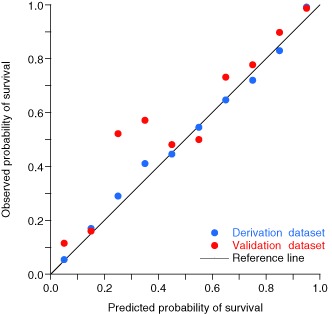
Eligible were patients admitted to Oslo University Hospital Ullevål within 24 h after injury with Injury Severity Score ≥ 10, proximal penetrating injuries or received by a trauma team. The derivation dataset comprised 5363 patients (August 2000 to July 2006); the validation dataset comprised 2517 patients (August 2006 to July 2008). Exclusion because of missing data was < 1%. Outcome was 30-day mortality. Logistic regression analysis incorporated fractional polynomial modelling and interaction effects. Model validation included a calibration plot, Hosmer-Lemeshow test and receiver operating characteristic (ROC) curves.
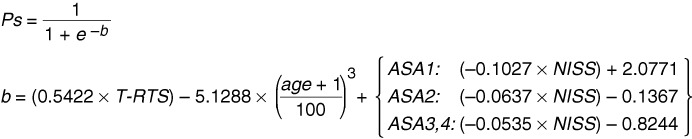
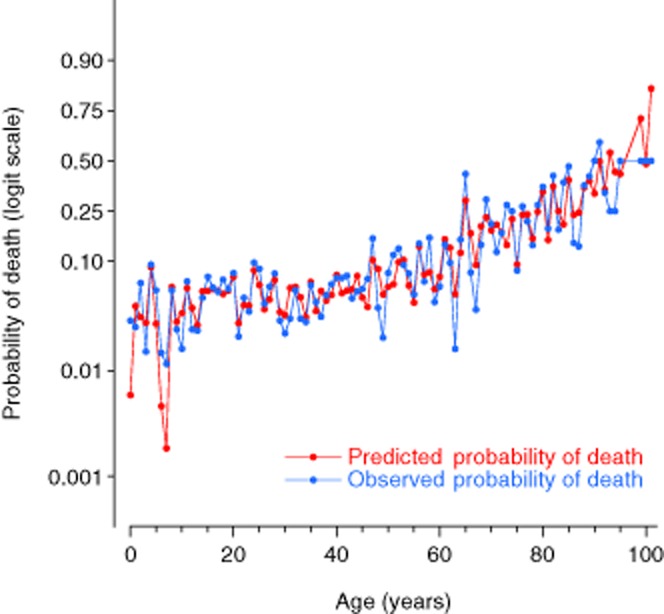
The new survival prediction model included the anatomic New Injury Severity Score (NISS), Triage Revised Trauma Score (T-RTS, comprising Glascow Coma Scale score, respiratory rate, and systolic blood pressure), age, pre-injury co-morbidity scored according to the American Society of Anesthesiologists Physical Status Classification System (ASA-PS), and an interaction term. Fractional polynomial analysis supported treating NISS and T-RTS as linear functions and age as cubic. Model discrimination between survivors and non-survivors was excellent. Area (95% confidence interval) under the ROC curve was 0.966 (0.959-0.972) in the derivation and 0.946 (0.930-0.962) in the validation dataset. Overall, low mortality and skewed survival probability distribution invalidated model calibration using the Hosmer-Lemeshow test.
The Norwegian survival prediction model in trauma (NORMIT) is a promising alternative to existing prediction models. External validation of the model in other trauma populations is warranted.
解剖损伤、生理紊乱、年龄和损伤机制是创伤预后的可靠预测指标。我们旨在开发并验证首个斯堪的纳维亚创伤生存预测模型。
纳入标准为伤后24小时内入住奥斯陆大学医院乌勒瓦尔分院、损伤严重度评分≥10分、近端穿透伤或由创伤团队接诊的患者。推导数据集包含5363例患者(2000年8月至2006年7月);验证数据集包含2517例患者(2006年8月至2008年7月)。因数据缺失而排除的患者<1%。结局指标为30天死亡率。逻辑回归分析采用分数多项式建模和交互效应。模型验证包括校准图、Hosmer-Lemeshow检验和受试者工作特征(ROC)曲线。
新的生存预测模型纳入了解剖学新损伤严重度评分(NISS)、分诊修正创伤评分(T-RTS,包括格拉斯哥昏迷量表评分、呼吸频率和收缩压)、年龄、根据美国麻醉医师协会身体状况分类系统(ASA-PS)评分的伤前合并症以及一个交互项。分数多项式分析支持将NISS和T-RTS视为线性函数,将年龄视为三次函数。模型对幸存者和非幸存者的区分能力极佳。推导数据集中ROC曲线下面积(95%置信区间)为0.966(0.959 - 0.972),验证数据集中为0.946(0.930 - 0.962)。总体而言,低死亡率和生存概率分布偏态使Hosmer-Lemeshow检验用于模型校准无效。
挪威创伤生存预测模型(NORMIT)是现有预测模型的一个有前景的替代方案。有必要在其他创伤人群中对该模型进行外部验证。