KEMRI-Wellcome Trust Research Programme, Centre for Geographic Medicine Research (Coast), Kilifi, Kenya.
Epilepsia. 2014 Feb;55(2):344-52. doi: 10.1111/epi.12498. Epub 2014 Jan 21.
The epilepsy treatment gap is largest in resource-poor countries. We evaluated the efficacy of a 1-day health education program in a rural area of Kenya. The primary outcome was adherence to antiepileptic drugs (AEDs) as measured by drug levels in the blood, and the secondary outcomes were seizure frequency and Kilifi Epilepsy Beliefs and Attitudes Scores (KEBAS).
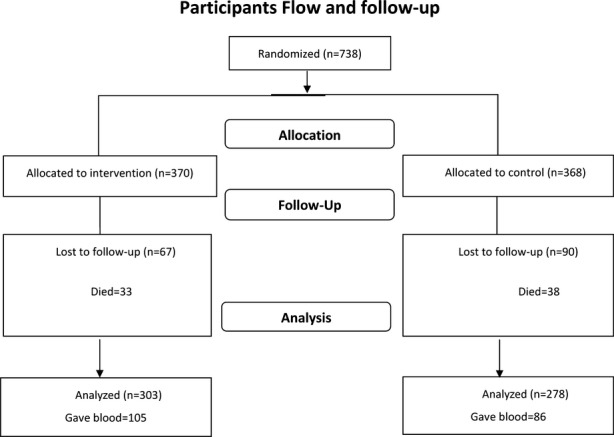
Seven hundred thirty-eight people with epilepsy (PWE) and their designated supporter were randomized to either the intervention (education) or nonintervention group. Data were collected at baseline and 1 year after the education intervention was administered to the intervention group. There were 581 PWE assessed at both time points. At the end of the study, 105 PWE from the intervention group and 86 from the nonintervention group gave blood samples, which were assayed for the most commonly used AEDs (phenobarbital, phenytoin, and carbamazepine). The proportions of PWE with detectable AED levels were determined using a standard blood assay method. The laboratory technicians conducting the assays were blinded to the randomization. Secondary outcomes were evaluated using questionnaires administered by trained field staff. Modified Poisson regression was used to investigate the factors associated with improved adherence (transition from nonoptimal AED level in blood at baseline to optimal levels at follow-up), reduced seizures, and improved KEBAS, which was done as a post hoc analysis. This trial is registered in ISRCTN register under ISRCTN35680481.
There was no significant difference in adherence to AEDs based on detectable drug levels (odds ratio [OR] 1.46, 95% confidence interval [95% CI] 0.74-2.90, p = 0.28) or by self-reports (OR 1.00, 95% CI 0.71-1.40, p = 1.00) between the intervention and nonintervention group. The intervention group had significantly fewer beliefs about traditional causes of epilepsy, cultural treatment, and negative stereotypes than the nonintervention group. There was no difference in seizure frequency. A comparison of the baseline and follow-up data showed a significant increase in adherence-intervention group (36-81% [p < 0.001]) and nonintervention group (38-74% [p < 0.001])-using detectable blood levels. The number of patients with less frequent seizures (≤3 seizures in the last 3 months) increased in the intervention group (62-80% [p = 0.002]) and in the nonintervention group (67-75% [p = 0.04]). Improved therapeutic adherence (observed in both groups combined) was positively associated with positive change in beliefs about risks of epilepsy (relative risk [RR] 2.00, 95% CI 1.03-3.95) and having nontraditional religious beliefs (RR 2.01, 95% CI 1.01-3.99). Reduced seizure frequency was associated with improved adherence (RR 1.72, 95% CI 1.19-2.47). Positive changes in KEBAS were associated with having tertiary education as compared to none (RR 1.09, 95% CI 1.05-1.14).
Health education improves knowledge about epilepsy, but once only contact does not improve adherence. However, sustained education may improve adherence in future studies.
癫痫治疗缺口在资源匮乏的国家最大。我们评估了在肯尼亚农村地区开展为期一天的健康教育计划的疗效。主要结局是通过血液中的药物水平来衡量抗癫痫药物(AED)的依从性,次要结局是癫痫发作频率和基利菲癫痫信念和态度评分(KEBAS)。
738 名癫痫患者(PWE)及其指定支持者被随机分配到干预(教育)或非干预组。在教育干预措施实施后 1 年收集基线和随访数据。共有 581 名 PWE 在两个时间点接受评估。研究结束时,干预组的 105 名 PWE 和非干预组的 86 名 PWE 提供了血样,这些血样用于检测最常用的 AED(苯巴比妥、苯妥英和卡马西平)。使用标准血药浓度检测方法确定有可检测 AED 水平的 PWE 的比例。进行检测的实验室技术人员对随机分组情况不知情。采用校正泊松回归分析调查与改善依从性(从基线时血液中非最佳 AED 水平过渡到随访时的最佳水平)、减少癫痫发作和改善 KEBAS 相关的因素,这是作为事后分析进行的。该试验在 ISRCTN 注册处注册,注册号为 ISRCTN35680481。
根据可检测药物水平(比值比[OR]1.46,95%置信区间[95%CI]0.74-2.90,p=0.28)或自我报告(OR1.00,95%CI0.71-1.40,p=1.00),干预组与非干预组之间的 AED 依从性无显著差异。与非干预组相比,干预组对癫痫传统病因、文化治疗和负面刻板印象的信念明显减少。癫痫发作频率无差异。对基线和随访数据的比较显示,干预组(36%-81%[p<0.001])和非干预组(38%-74%[p<0.001])的依从性显著增加,均采用可检测的血药水平。癫痫发作次数较少(过去 3 个月内≤3 次发作)的患者数量在干预组(62%-80%[p=0.002])和非干预组(67%-75%[p=0.04])中增加。治疗依从性的改善(在两组中均观察到)与对癫痫风险的信念的积极变化呈正相关(相对风险[RR]2.00,95%CI1.03-3.95)和具有非传统宗教信仰(RR2.01,95%CI1.01-3.99)。癫痫发作频率降低与依从性改善相关(RR1.72,95%CI1.19-2.47)。KEBAS 的积极变化与接受高等教育(与没有接受相比)呈正相关(RR1.09,95%CI1.05-1.14)。
健康教育可提高对癫痫的认识,但仅一次接触并不能提高依从性。然而,持续的教育可能会在未来的研究中提高依从性。