Schmidt Matthieu, Pellegrino Vincent, Combes Alain, Scheinkestel Carlos, Cooper D Jamie, Hodgson Carol
Crit Care. 2014 Jan 21;18(1):203. doi: 10.1186/cc13702.
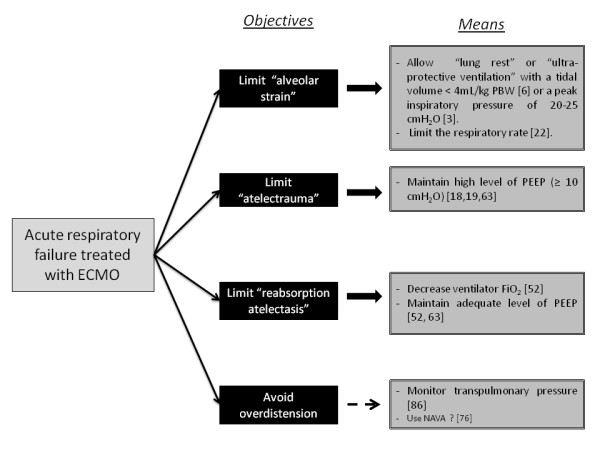
The timing of extracorporeal membrane oxygenation (ECMO) initiation and its outcome in the management of respiratory and cardiac failure have received considerable attention, but very little attention has been given to mechanical ventilation during ECMO. Mechanical ventilation settings in non-ECMO studies have been shown to have an effect on survival and may also have contributed to a treatment effect in ECMO trials. Protective lung ventilation strategies established for non-ECMO-supported respiratory failure patients may not be optimal for more severe forms of respiratory failure requiring ECMO support. The influence of positive end-expiratory pressure on the reduction of the left ventricular compliance may be a matter of concern for patients receiving ECMO support for cardiac failure. The objectives of this review were to describe potential mechanisms for lung injury during ECMO for respiratory or cardiac failure, to assess the possible benefits from the use of ultra-protective lung ventilation strategies and to review published guidelines and expert opinions available on mechanical ventilation-specific management of patients requiring ECMO, including mode and ventilator settings. Articles were identified through a detailed search of PubMed, Ovid, Cochrane databases and Google Scholar. Additional references were retrieved from the selected studies. Growing evidence suggests that mechanical ventilation settings are important in ECMO patients to minimize further lung damage and improve outcomes. An ultra-protective ventilation strategy may be optimal for mechanical ventilation during ECMO for respiratory failure. The effects of airway pressure on right and left ventricular afterload should be considered during venoarterial ECMO support of cardiac failure. Future studies are needed to better understand the potential impact of invasive mechanical ventilation modes and settings on outcomes.
体外膜肺氧合(ECMO)启动的时机及其在呼吸和心力衰竭管理中的结果已受到相当多的关注,但ECMO期间的机械通气却很少受到关注。非ECMO研究中的机械通气设置已被证明对生存率有影响,并且可能也对ECMO试验中的治疗效果有贡献。为非ECMO支持的呼吸衰竭患者建立的肺保护性通气策略对于需要ECMO支持的更严重形式的呼吸衰竭可能并非最佳。呼气末正压对左心室顺应性降低的影响可能是接受ECMO支持治疗心力衰竭患者需要关注的问题。本综述的目的是描述呼吸或心力衰竭患者在ECMO期间肺损伤的潜在机制,评估使用超保护性肺通气策略可能带来的益处,并回顾已发表的关于需要ECMO患者机械通气特定管理的指南和专家意见,包括模式和呼吸机设置。通过对PubMed、Ovid、Cochrane数据库和谷歌学术进行详细检索来确定文章。从选定的研究中检索其他参考文献。越来越多的证据表明,机械通气设置对于ECMO患者至关重要,可将进一步的肺损伤降至最低并改善预后。对于呼吸衰竭患者在ECMO期间进行机械通气,超保护性通气策略可能是最佳的。在心力衰竭的静脉 - 动脉ECMO支持期间,应考虑气道压力对右心室和左心室后负荷的影响。需要未来的研究来更好地了解有创机械通气模式和设置对预后的潜在影响。