van den Hoven Andor F, Smits Maarten L J, Rosenbaum Charlotte E N M, Verkooijen Helena M, van den Bosch Maurice A A J, Lam Marnix G E H
Department of Radiology and Nuclear Medicine, University Medical Center Utrecht, Utrecht, The Netherlands.
PLoS One. 2014 Jan 17;9(1):e86394. doi: 10.1371/journal.pone.0086394. eCollection 2014.
Treatment efficacy of intra-arterial radioembolization for liver tumors depends on the selective targeting of tumorous tissue. Recent investigations have demonstrated that tumors may receive inadequate doses of radioactivity after radioembolization, due to unfavorable tumor to non-tumor (T/N) uptake ratios of radioactive microspheres. Hepatic arterial infusion of the vasoconstrictor angiotensin II (AT-II) is reported to increase the T/N blood flow ratio. The purpose of this systematic review was to provide a comprehensive overview of the effect of hepatic arterial AT-II on T/N blood flow ratio in patients with hepatic malignancies, and determine its clinical value for radioembolization.
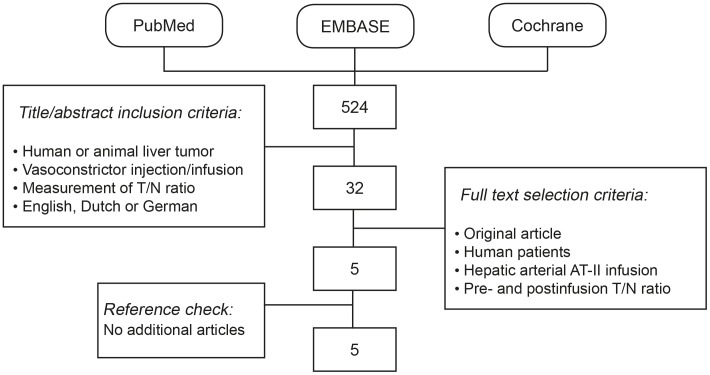
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A structured search was performed in the PubMed, EMBASE and Cochrane databases. Only studies that presented data on T/N ratios before and after infusion of AT-II into the hepatic artery, in human patients with hepatic malignancies, were selected. Median T/N ratios before, during and after AT-II infusion, and the median T/N ratio improvement factor were extracted from the selected articles. All data on systemic blood pressure measurements and clinical symptoms were also extracted.
The search identified 524 titles of which 5 studies, including a total of 71 patients were considered relevant. Median T/N ratios before infusion of AT-II ranged from 0.4 to 3.4. All studies observed a substantial improvement of the T/N ratio after AT-II infusion, with median improvement factors ranging from 1.8 to 3.1. A transitory increase of systemic blood pressure was observed during AT-II infusion.
Infusion of AT-II into the hepatic artery leads to an increase of the tumor to non-tumor blood flow ratio, as measured by T/N uptake ratios. Clinical trials are warranted to assess safety aspects, optimal administration strategy and impact on treatment efficacy during radioembolization.
肝肿瘤动脉内放射性栓塞治疗的疗效取决于对肿瘤组织的选择性靶向。最近的研究表明,由于放射性微球的肿瘤与非肿瘤(T/N)摄取率不理想,放射性栓塞后肿瘤可能接受的放射性剂量不足。据报道,肝动脉输注血管收缩剂血管紧张素II(AT-II)可提高T/N血流比。本系统评价的目的是全面概述肝动脉AT-II对肝恶性肿瘤患者T/N血流比的影响,并确定其在放射性栓塞中的临床价值。
本评价按照系统评价和Meta分析的首选报告项目指南进行。在PubMed、EMBASE和Cochrane数据库中进行了结构化检索。仅选择了在肝恶性肿瘤患者肝动脉内输注AT-II前后提供T/N比数据的研究。从选定的文章中提取AT-II输注前、输注期间和输注后的T/N比中位数,以及T/N比改善因子中位数。还提取了所有关于全身血压测量和临床症状的数据。
检索到524个标题,其中5项研究(共71例患者)被认为相关。AT-II输注前的T/N比中位数为0.4至3.4。所有研究均观察到AT-II输注后T/N比有显著改善,改善因子中位数为1.8至3.1。在AT-II输注期间观察到全身血压短暂升高。
肝动脉内输注AT-II可导致肿瘤与非肿瘤血流比增加,以T/N摄取率衡量。有必要进行临床试验,以评估放射性栓塞期间的安全性、最佳给药策略以及对治疗效果的影响。