Char Jessica E, Wolfe Marlene H, Cho Hyung-Ju, Park Il-Ho, Jeong Jin Hyeok, Frisbee Eric, Dunn Colleen, Davies Zoe, Milla Carlos, Moss Richard B, Thomas Ewart A C, Wine Jeffrey J
Cystic Fibrosis Research Laboratory, Stanford University, Stanford, California, United States of America.
Department of Pediatrics, Stanford University School of Medicine, Stanford, California, United States of America.
PLoS One. 2014 Feb 10;9(2):e88564. doi: 10.1371/journal.pone.0088564. eCollection 2014.
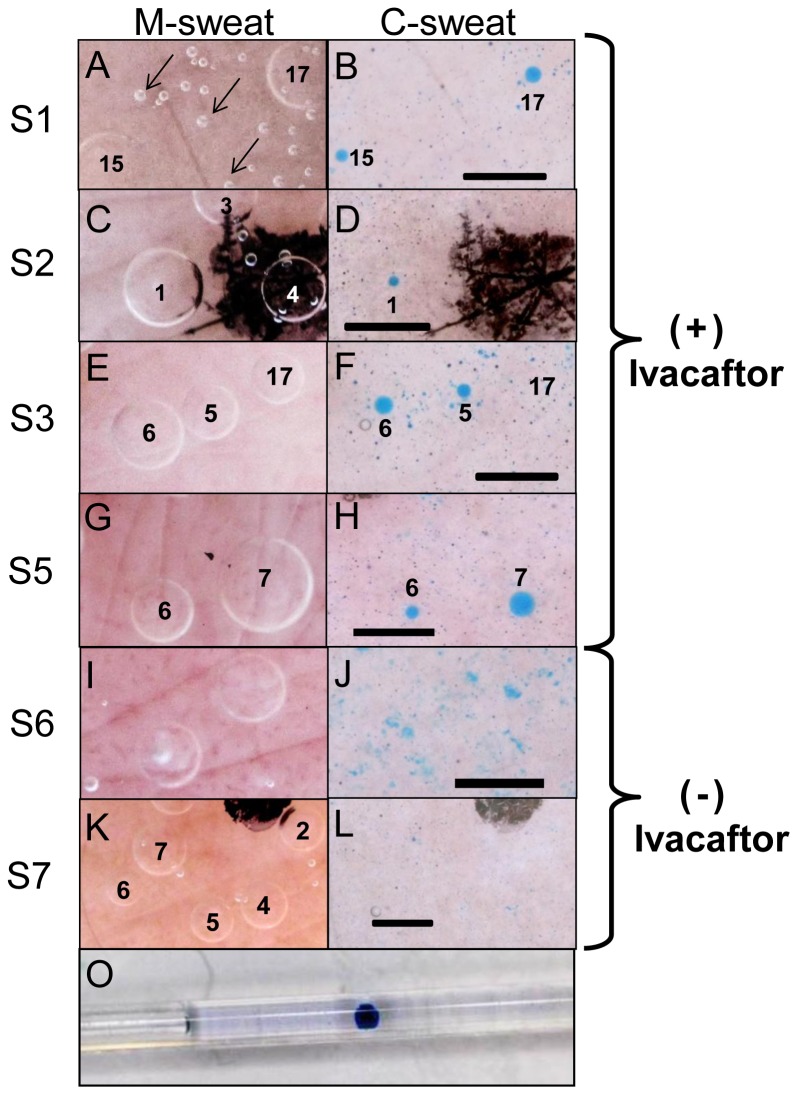
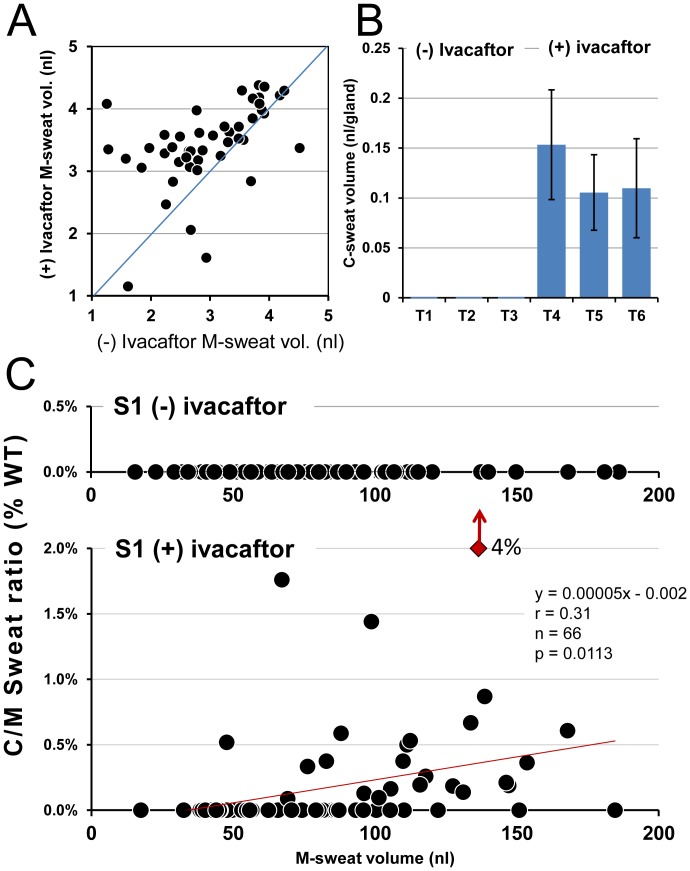
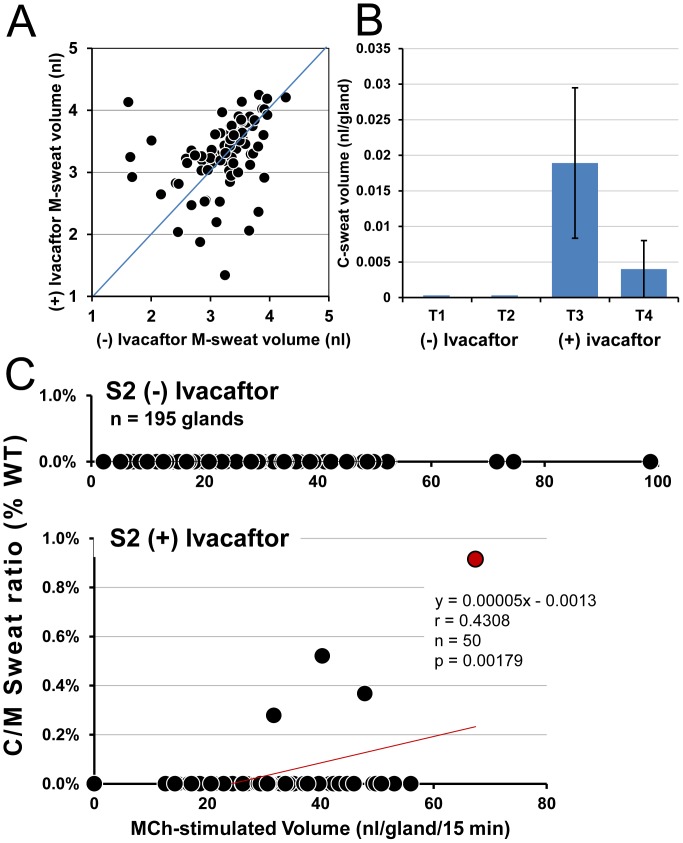
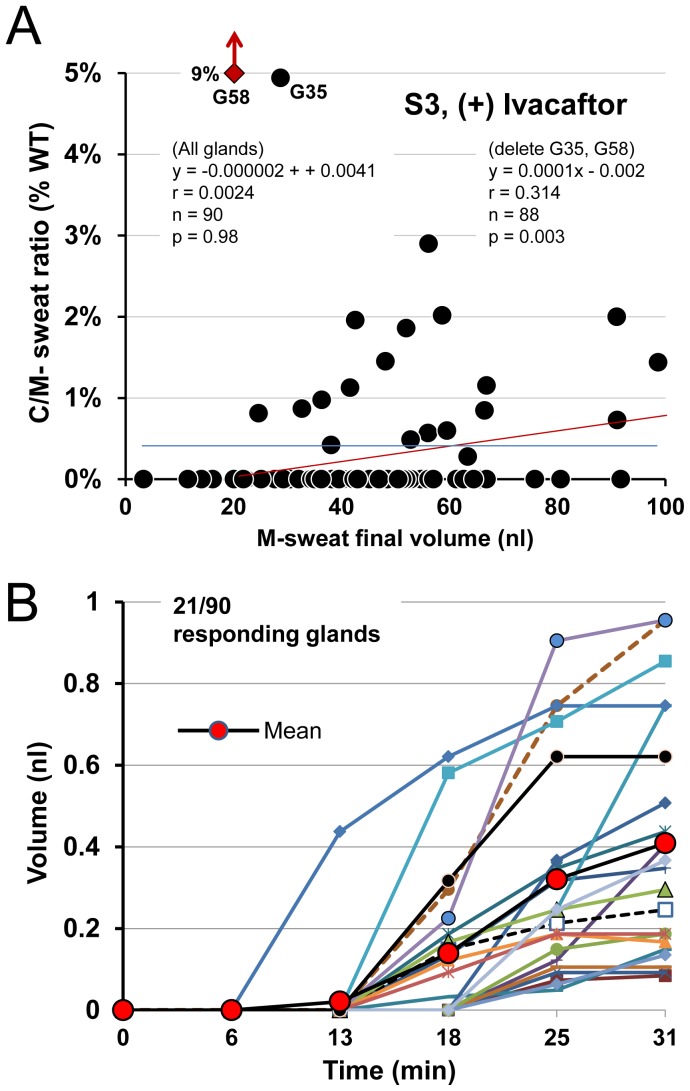
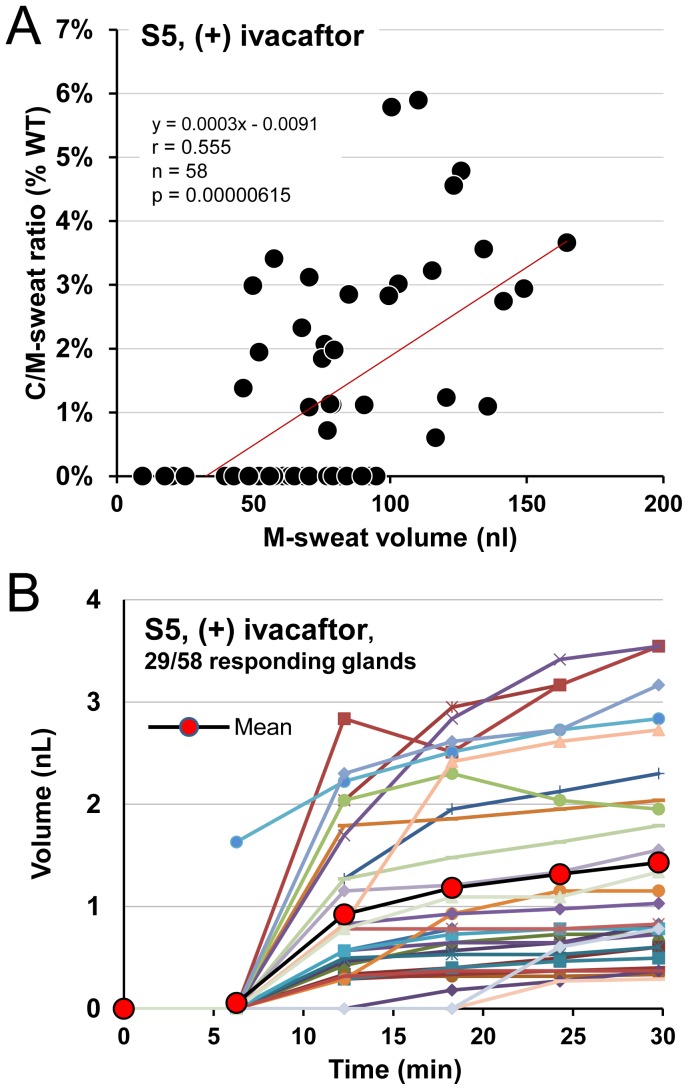
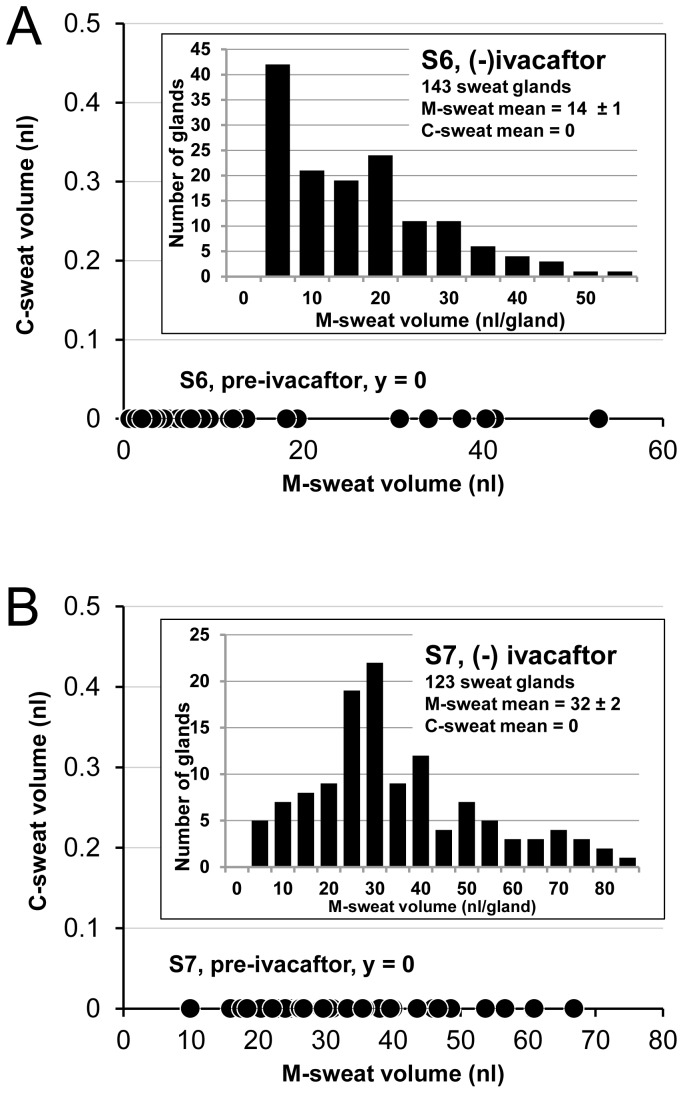
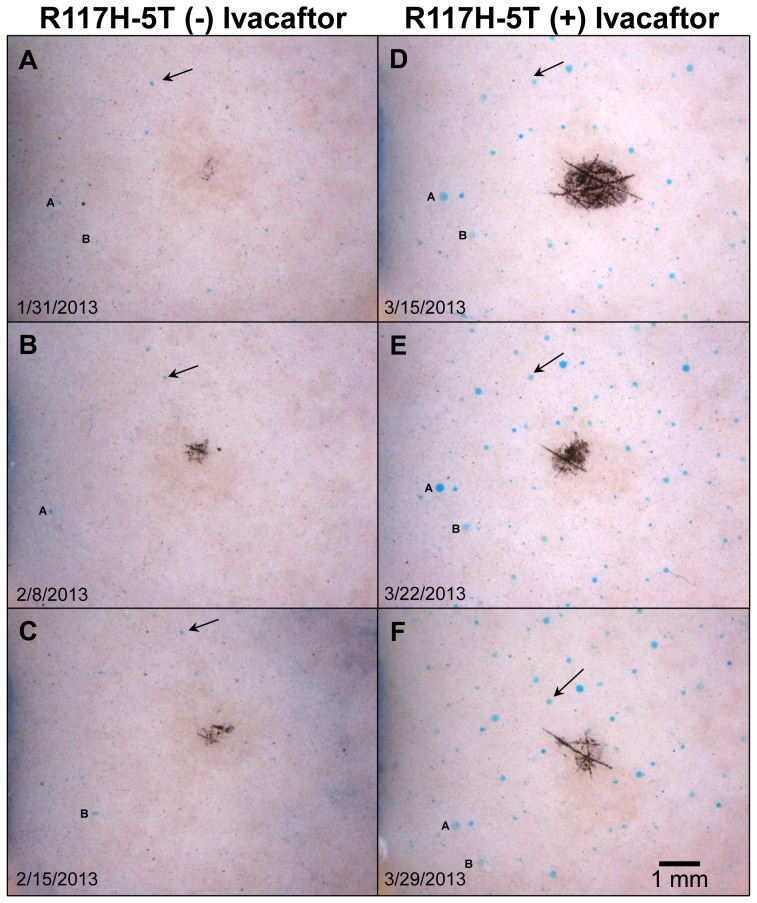
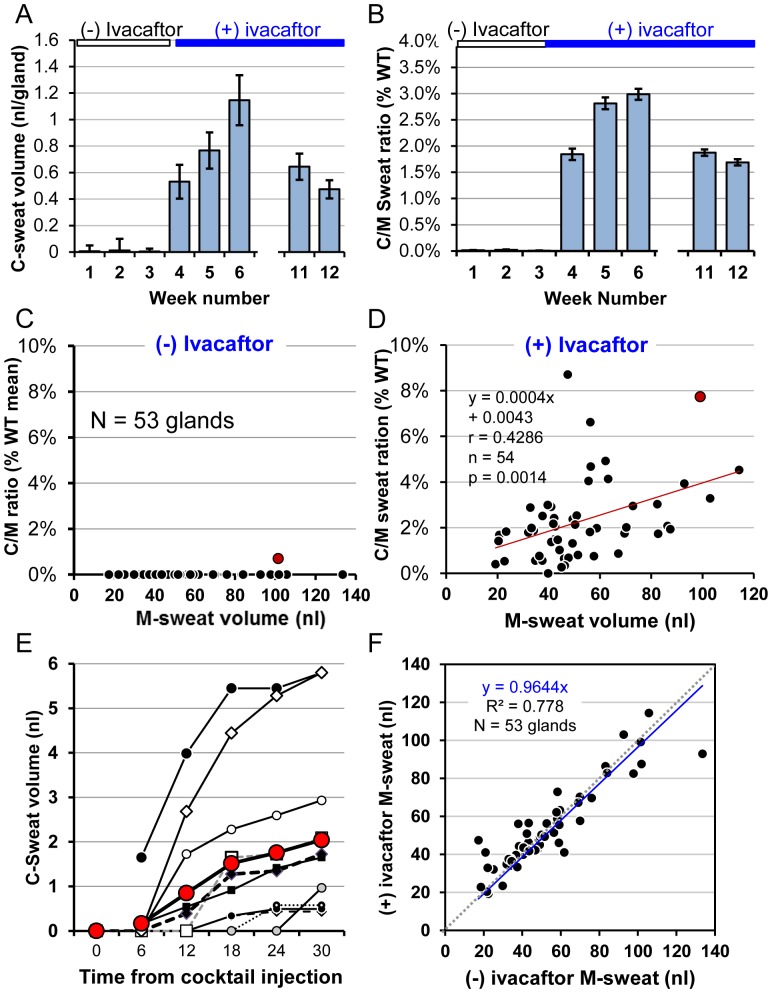
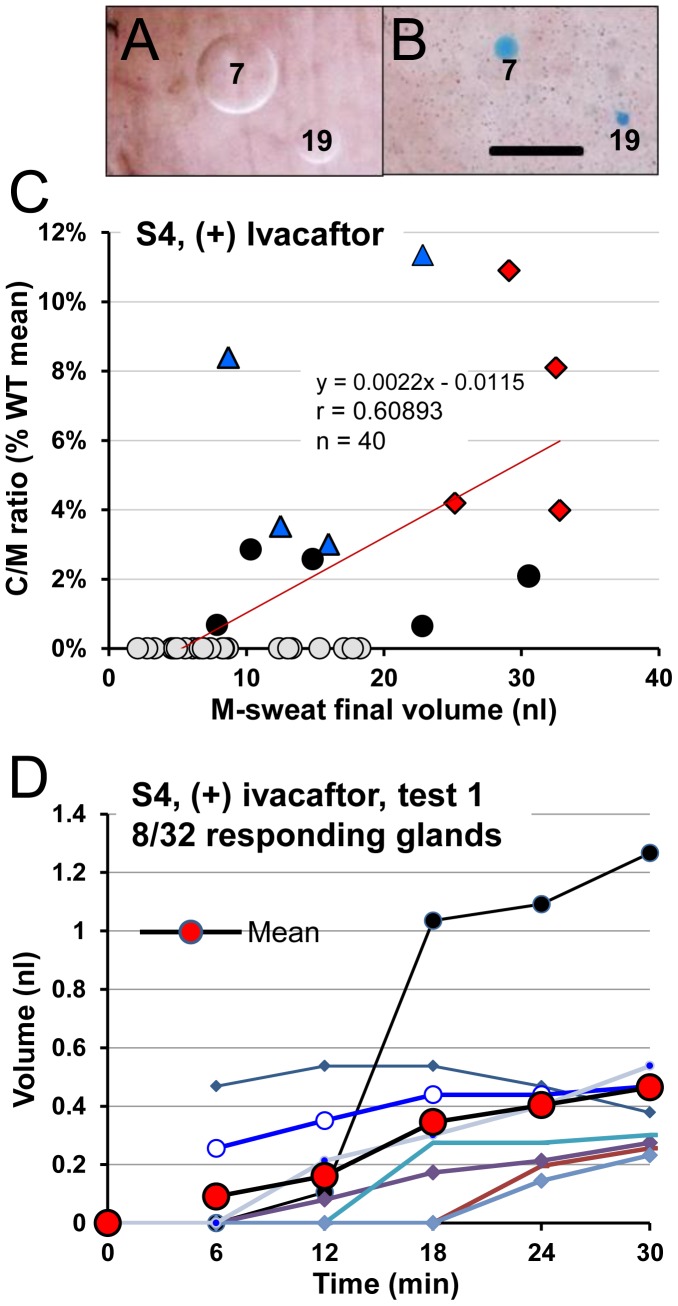
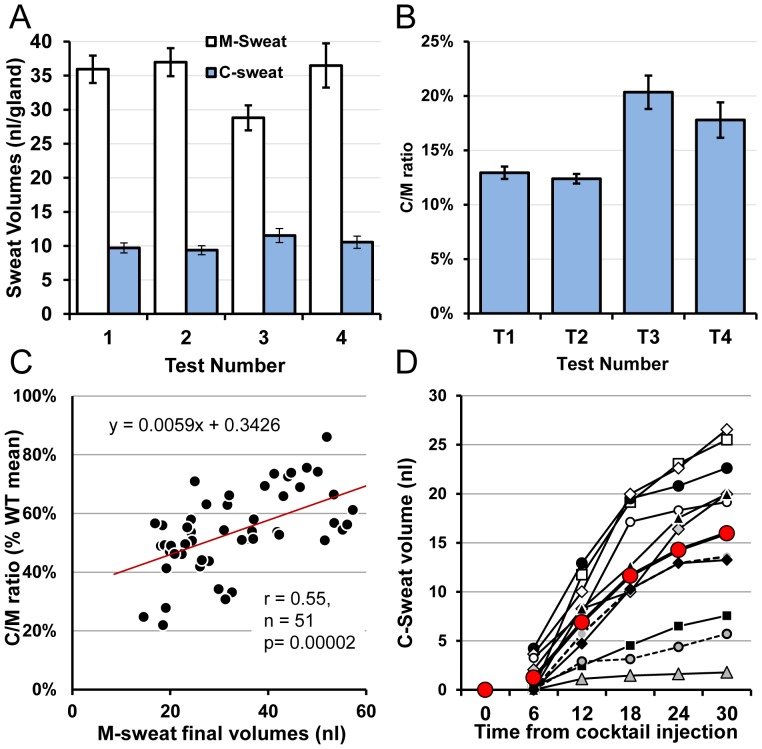
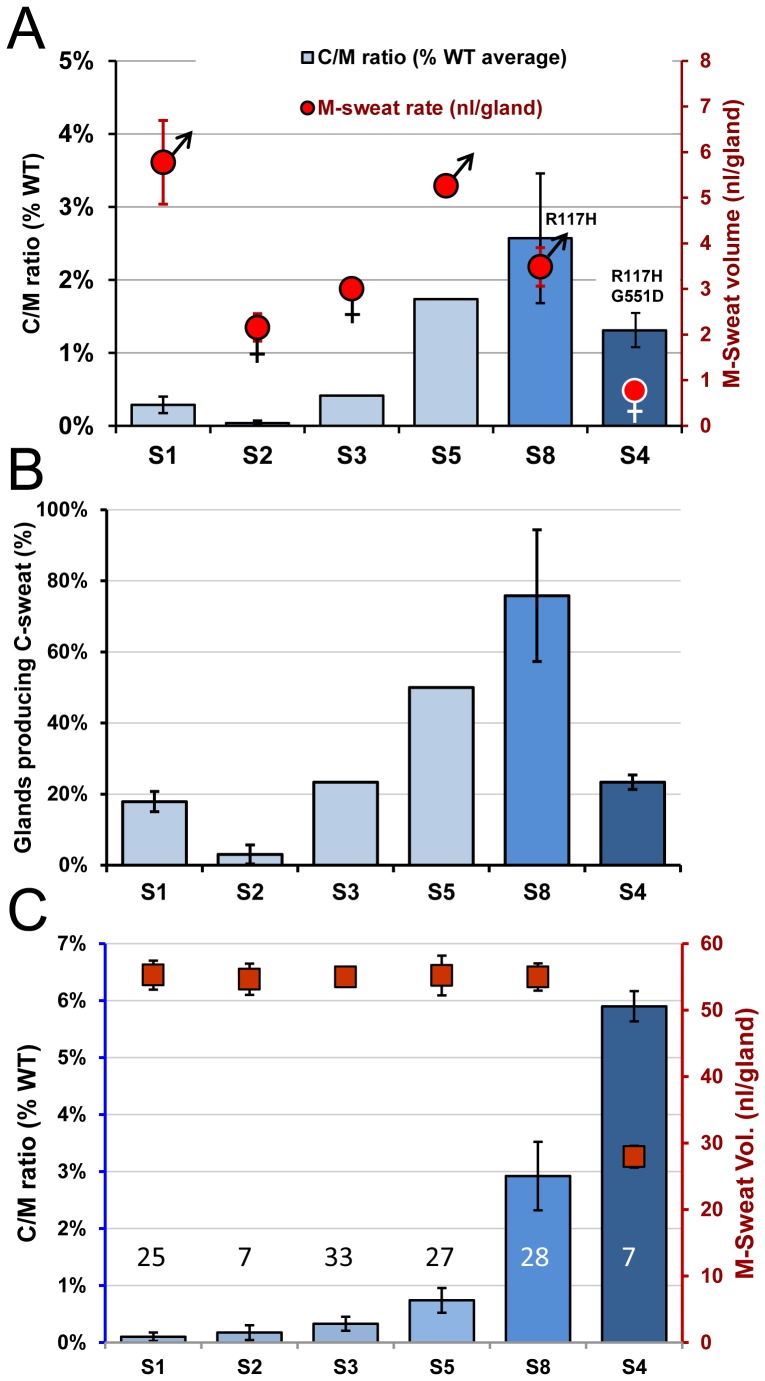
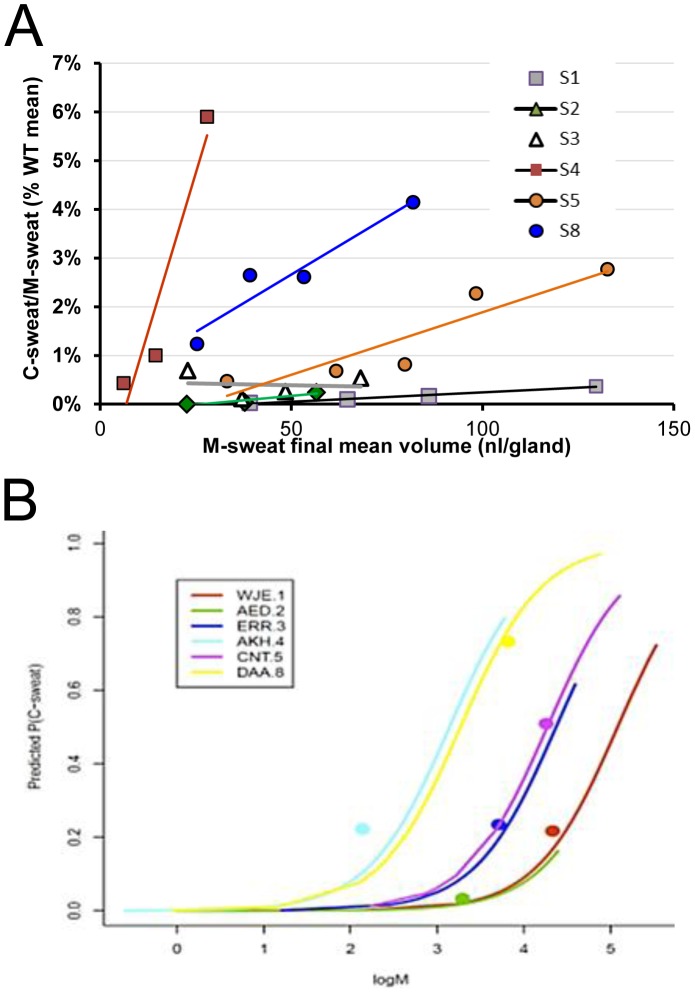
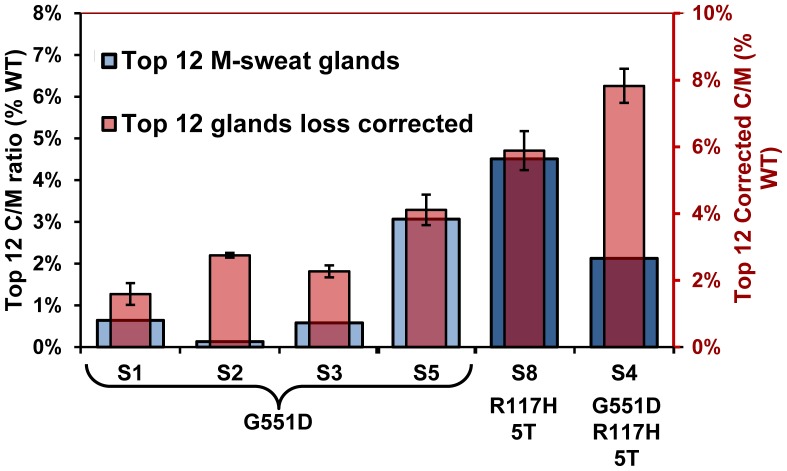
To determine if oral dosing with the CFTR-potentiator ivacaftor (VX-770, Kalydeco) improves CFTR-dependent sweating in CF subjects carrying G551D or R117H-5T mutations, we optically measured sweat secretion from 32-143 individually identified glands in each of 8 CF subjects; 6 F508del/G551D, one G551D/R117H-5T, and one I507del/R117H-5T. Two subjects were tested only (-) ivacaftor, 3 only (+) ivacaftor and 3 (+/-) ivacaftor (1-5 tests per condition). The total number of gland measurements was 852 (-) ivacaftor and 906 (+) ivacaftor. A healthy control was tested 4 times (51 glands). For each gland we measured both CFTR-independent (M-sweat) and CFTR-dependent (C-sweat); C-sweat was stimulated with a β-adrenergic cocktail that elevated [cAMP]i while blocking muscarinic receptors. Absent ivacaftor, almost all CF glands produced M-sweat on all tests, but only 1/593 glands produced C-sweat (10 tests, 5 subjects). By contrast, 6/6 subjects (113/342 glands) produced C-sweat in the (+) ivacaftor condition, but with large inter-subject differences; 3-74% of glands responded with C/M sweat ratios 0.04%-2.57% of the average WT ratio of 0.265. Sweat volume losses cause proportionally larger underestimates of CFTR function at lower sweat rates. The losses were reduced by measuring C/M ratios in 12 glands from each subject that had the highest M-sweat rates. Remaining losses were estimated from single channel data and used to correct the C/M ratios, giving estimates of CFTR function (+) ivacaftor = 1.6%-7.7% of the WT average. These estimates are in accord with single channel data and transcript analysis, and suggest that significant clinical benefit can be produced by low levels of CFTR function.
为了确定口服CFTR增强剂依伐卡托(VX - 770,凯力迪科)是否能改善携带G551D或R117H - 5T突变的囊性纤维化(CF)患者中CFTR依赖的出汗情况,我们通过光学方法测量了8名CF患者中每个患者32 - 143个单独识别的汗腺的汗液分泌;其中6名F508del/G551D患者,1名G551D/R117H - 5T患者,1名I507del/R117H - 5T患者。2名受试者仅接受了依伐卡托阴性测试,3名仅接受了依伐卡托阳性测试,3名接受了依伐卡托阳性和阴性测试(每种情况进行1 - 5次测试)。汗腺测量的总数为依伐卡托阴性时852次,依伐卡托阳性时906次。一名健康对照者接受了4次测试(51个汗腺)。对于每个汗腺,我们测量了CFTR非依赖的(M - 汗液)和CFTR依赖的(C - 汗液);通过一种β - 肾上腺素能混合剂刺激C - 汗液分泌,该混合剂可升高细胞内[环磷酸腺苷](cAMP)水平,同时阻断毒蕈碱受体。在没有依伐卡托的情况下,几乎所有CF汗腺在所有测试中都产生M - 汗液,但只有1/593个汗腺产生C - 汗液(10次测试,5名受试者)。相比之下 在依伐卡托阳性的情况下,6/6名受试者(113/342个汗腺)产生了C - 汗液,但受试者之间差异很大;3%至74%的汗腺对C/M汗液比值的反应为平均野生型(WT)比值0.265的0.04% - 2.57%。在较低的出汗率下,汗液量的损失会导致对CFTR功能的低估比例更大。通过测量每个受试者中M - 汗液率最高的12个汗腺的C/M比值,减少了这些损失。根据单通道数据估计剩余损失,并用于校正C/M比值,得出依伐卡托阳性时CFTR功能的估计值为野生型平均值的1.6% - 7.7%。这些估计值与单通道数据和转录分析结果一致,并表明低水平的CFTR功能也能产生显著的临床益处。