Ross Ian Louis, Bergthorsdottir Ragnhildur, Levitt Naomi, Dave Joel Alex, Schatz Desmond, Marais David, Johannsson Gudmundur
Division of Endocrinology, Department of Medicine, University of Cape Town, Cape Town, South Africa.
Department of Endocrinology, Institute of Medicine, Sahlgrenska University Hospital, University of Gothenburg, Gothenburg, Sweden.
PLoS One. 2014 Mar 6;9(6):e90768. doi: 10.1371/journal.pone.0090768. eCollection 2014.
Patients with Addison's disease (AD) in Scandinavia have an increased risk for premature death due to cardiovascular disease (CVD). Serum lipids are important risk factors for CVD and vascular mortality. Replacement doses of hydrocortisone have historically been higher in Sweden than South Africa. The primary aim was to study the lipid profiles in a large group of patients with AD with the hypothesis that the lipid profile in patients in Sweden would be worse than in South Africa.
In a cross-sectional study, 110 patients with AD (55 from South Africa, 55 from Sweden) matched for age, gender, ethnicity and BMI were studied. Anthropometric measures, blood pressure, lipids, highly sensitive C-reactive protein (hs-CRP) and adiponectin were studied.
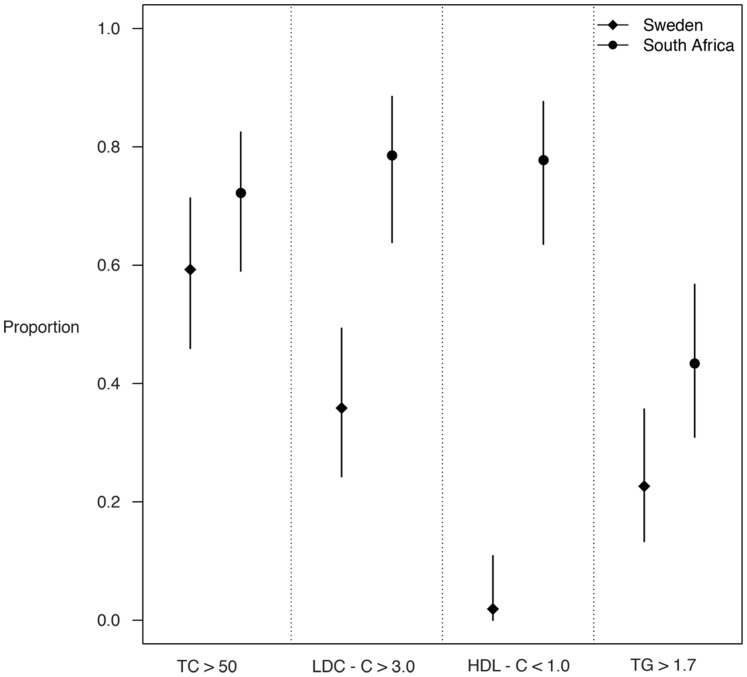
All patients were Caucasian and the majority were women N = 36 (65.5%). Mean (standard deviation; SD) ages of the Swedish and South African patients were 52.9 (13.0) and 52.6 (14.4) years and BMI 25.3 (3.2) and 25.8 (4.1) kg/m2, respectively. The mean total daily hydrocortisone dose was greater in the Swedish patients than the South African patients, [33.0 (8.1) versus 24.3 (8.0) mg; p<0.0001]. South African patients had higher median (interquartilerange; IQR) triglycerides (TG) [1.59 (1.1-2.46) versus 0.96 (0.74-1.6) mmol/l; p<0.001], total cholesterol (TC) [6.02(1.50) versus 5.13 (0.87) mmol/l; p<0.001], LDL-C [4.43 (1.44) versus 2.75 (0.80) mmol/l; p<0.001] and median hs-CRP [2.15 (0.93-5.45) versus 0.99 (0.57-2.10) mg/L; p<0.003] and lower HDL-C [0.80 (0.40) versus 1.86 (0.46) mmol/l; p<0.001] than the Swedish patients. Approximately 20% of the patients in both cohorts had hypertension and diabetes mellitus.
South African patients with AD have worse lipid profiles and higher hs-CRP compared to their matched Swedish patients, despite lower doses of hydrocortisone. It is uncertain at this time whether these are due to genetic or environmental factors.
斯堪的纳维亚地区的艾迪生病(AD)患者因心血管疾病(CVD)导致过早死亡的风险增加。血清脂质是CVD和血管性死亡的重要危险因素。瑞典历史上氢化可的松的替代剂量高于南非。主要目的是研究一大群AD患者的血脂谱,假设瑞典患者的血脂谱比南非患者更差。
在一项横断面研究中,对110例年龄、性别、种族和体重指数相匹配的AD患者(55例来自南非,55例来自瑞典)进行了研究。研究了人体测量指标、血压、血脂、高敏C反应蛋白(hs-CRP)和脂联素。
所有患者均为白种人,大多数为女性,N = 36(65.5%)。瑞典和南非患者的平均(标准差;SD)年龄分别为52.9(13.0)岁和52.6(14.4)岁,体重指数分别为25.3(3.2)和25.8(4.1)kg/m²。瑞典患者的平均每日氢化可的松总剂量高于南非患者,[33.0(8.1)对24.3(8.0)mg;p<0.0001]。南非患者的甘油三酯(TG)中位数(四分位间距;IQR)[1.59(1.1 - 2.46)对0.96(0.74 - 1.6)mmol/l;p<0.001]、总胆固醇(TC)[6.02(1.50)对5.13(0.87)mmol/l;p<0.001]、低密度脂蛋白胆固醇(LDL-C)[4.43(1.44)对2.75(0.80)mmol/l;p<0.001]和hs-CRP中位数[2.15(0.93 - 5.45)对0.99(0.57 - 2.10)mg/L;p<0.003]均高于瑞典患者,而高密度脂蛋白胆固醇(HDL-C)[0.80(0.40)对1.86(0.46)mmol/l;p<0.001]低于瑞典患者。两个队列中约20%的患者患有高血压和糖尿病。
与匹配的瑞典患者相比,南非AD患者的血脂谱更差,hs-CRP更高,尽管氢化可的松剂量较低。目前尚不确定这些是由遗传因素还是环境因素导致的。