*Department of Surgery, University of Toronto, Toronto, Ontario, Canada †Department of Internal Medicine, Mount Sinai Hospital, New York City, NY ‡Department of Surgery, McGill University, Montreal, Quebec, Canada §Department of Internal Medicine, University of Toronto, Toronto, Ontario, Canada ‖Department of Critical Care Medicine, University of Toronto, Toronto, Ontario, Canada ¶Department of Surgery, University of British Columbia, Vancouver, British Columbia, Canada **Department of Surgery, Royal Inland Hospital, Kamloops, British Columbia, Canada.
Ann Surg. 2014 Jun;259(6):1041-53. doi: 10.1097/SLA.0000000000000595.
In 2003, the Accreditation Council for Graduate Medical Education (ACGME) mandated 80-hour resident duty limits. In 2011 the ACGME mandated 16-hour duty maximums for PGY1 (post graduate year) residents. The stated goals were to improve patient safety, resident well-being, and education. A systematic review and meta-analysis were performed to evaluate the impact of resident duty hours (RDH) on clinical and educational outcomes in surgery.
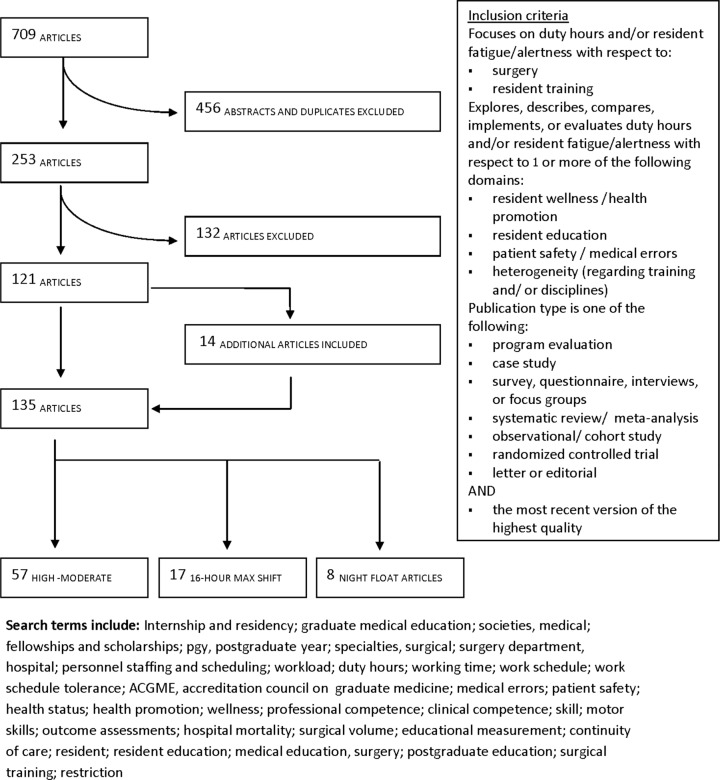
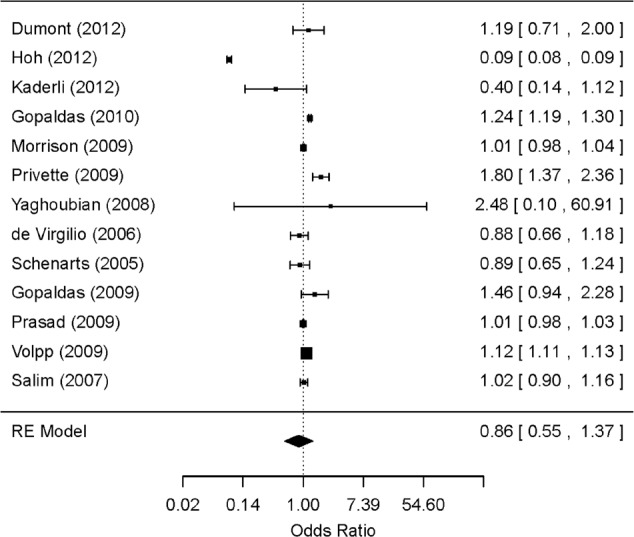
A systematic review (1980-2013) was executed on CINAHL, Cochrane Database, Embase, Medline, and Scopus. Quality of articles was assessed using the GRADE guidelines. Sixteen-hour shifts and night float systems were analyzed separately. Articles that examined mortality data were combined in a random-effects meta-analysis to evaluate the impact of RDH on patient mortality.
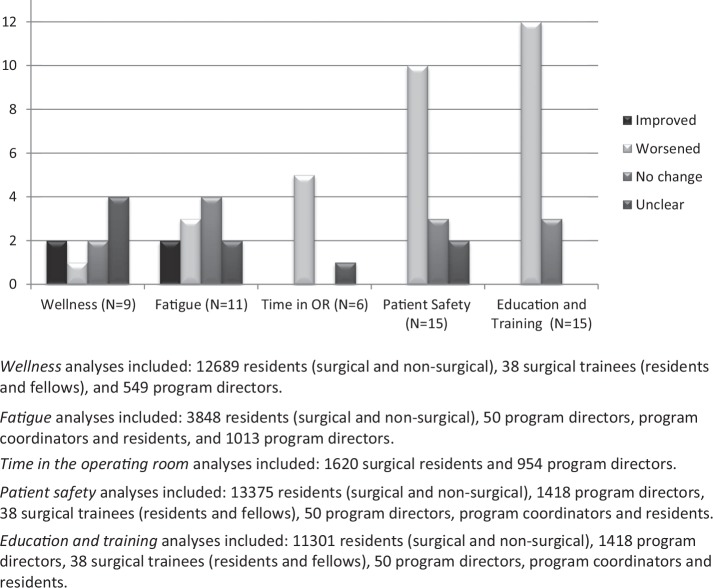
A total of 135 articles met the inclusion criteria. Among these, 42% (N = 57) were considered moderate-high quality. There was no overall improvement in patient outcomes as a result of RDH; however, some studies suggest increased complication rates in high-acuity patients. There was no improvement in education related to RDH restrictions, and performance on certification examinations has declined in some specialties. Survey studies revealed a perception of worsened education and patient safety. There were improvements in resident wellness after the 80-hour workweek, but there was little improvement or negative effects on wellness after 16-hour duty maximums were implemented.
Recent RDH changes are not consistently associated with improvements in resident well-being, and have negative impacts on patient outcomes and performance on certification examinations. Greater flexibility to accommodate resident training needs is required. Further erosion of training time should be considered with great caution.
2003 年,美国毕业后医学教育认证委员会(ACGME)规定住院医师的工作时间限制为 80 小时。2011 年,ACGME 规定住院医师第一年(PGY1)的工作时间上限为 16 小时。其设定的目标是提高患者安全、住院医师的幸福感和教育质量。本系统回顾和荟萃分析旨在评估住院医师工作时间(RDH)对手术的临床和教育结果的影响。
在 CINAHL、Cochrane 数据库、Embase、Medline 和 Scopus 上进行了系统的文献检索(1980-2013 年)。使用 GRADE 指南评估文章的质量。单独分析了 16 小时轮班和夜班轮休制度。将研究死亡率数据的文章合并进行随机效应荟萃分析,以评估 RDH 对患者死亡率的影响。
共有 135 篇文章符合纳入标准。其中,42%(N=57)被认为是质量较高的。RDH 并没有总体改善患者的预后,但一些研究表明,高风险患者的并发症发生率有所增加。RDH 限制并没有改善教育相关内容,而且一些专业的认证考试成绩有所下降。调查研究显示,住院医师的教育和患者安全状况恶化。实施每周 80 小时工作时间限制后,住院医师的幸福感有所提高,但实施 16 小时工作时间上限后,幸福感几乎没有改善或产生负面影响。
最近的 RDH 变化并不总是与住院医师的幸福感改善相关,反而对患者的预后和认证考试成绩产生负面影响。需要有更大的灵活性来满足住院医师的培训需求。进一步减少培训时间应慎重考虑。