Auer Reto, Gencer Baris, Räber Lorenz, Klingenberg Roland, Carballo Sebastian, Carballo David, Nanchen David, Cornuz Jacques, Vader John-Paul, Vogt Pierre, Jüni Peter, Matter Christian M, Windecker Stephan, Lüscher Thomas Felix, Mach François, Rodondi Nicolas
Department of Epidemiology and Biostatistics, UCSF, San Francisco, California, United States of America.
Division of Cardiology, Faculty of Medicine, Geneva University Hospitals, Geneva, Switzerland.
PLoS One. 2014 Mar 27;9(3):e93147. doi: 10.1371/journal.pone.0093147. eCollection 2014.
Adherence to guidelines is associated with improved outcomes of patients with acute coronary syndrome (ACS). Clinical registries developed to assess quality of care at discharge often do not collect the reasons for non-prescription for proven efficacious preventive medication in Continental Europe. In a prospective cohort of patients hospitalized for an ACS, we aimed at measuring the rate of recommended treatment at discharge, using pre-specified quality indicators recommended in cardiologic guidelines and including systematic collection of reasons for non-prescription for preventive medications.
In a prospective cohort with 1260 patients hospitalized for ACS, we measured the rate of recommended treatment at discharge in 4 academic centers in Switzerland. Performance measures for medication at discharge were pre-specified according to guidelines, systematically collected for all patients and included in a centralized database.
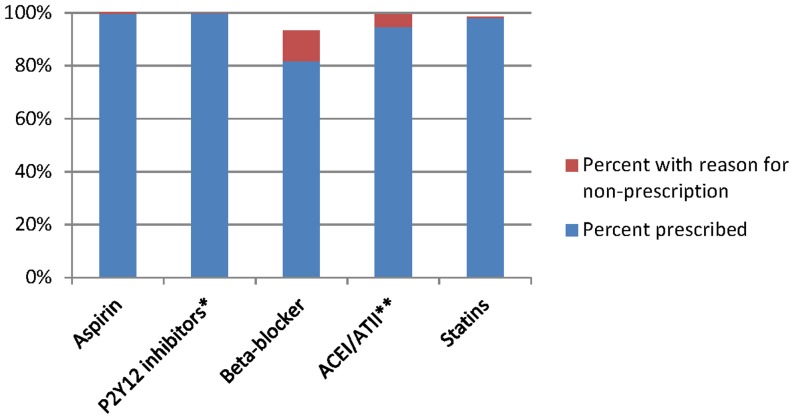
Six hundred and eighty eight patients(54.6%) were discharged with a main diagnosis of STEMI, 491(39%) of NSTEMI and 81(6.4%) of unstable angina. Mean age was 64 years and 21.3% were women. 94.6% were prescribed angiotensin converting enzyme inhibitors/angiotensin II receptor blockers at discharge when only considering raw prescription rates, but increased to 99.5% when including reasons non-prescription. For statins, rates increased from 98% to 98.6% when including reasons for non-prescription and for beta-blockers, from 82% to 93%. For aspirin, rates further increased from 99.4% to 100% and from to 99.8% to 100% for P2Y12 inhibitors.
We found a very high adherence to ACS guidelines for drug prescriptions at discharge when including reasons for non-prescription to drug therapy. For beta-blockers, prescription rates were suboptimal, even after taking into account reason for non-prescription. In an era of improving quality of care to achieve 100% prescription rates at discharge unless contra-indicated, pre-specification of reasons for non-prescription for cardiovascular preventive medication permits to identify remaining gaps in quality of care at discharge.
ClinicalTrials.gov NCT01000701.
遵循指南与急性冠脉综合征(ACS)患者预后改善相关。在欧洲大陆,为评估出院时医疗质量而建立的临床登记系统通常不收集未开具已证实有效的预防性药物的原因。在一个因ACS住院的前瞻性队列患者中,我们旨在使用心脏病学指南中推荐的预先设定的质量指标,包括系统收集预防性药物未处方的原因,来衡量出院时推荐治疗的比例。
在一个有1260例因ACS住院患者的前瞻性队列中,我们在瑞士的4个学术中心测量了出院时推荐治疗的比例。出院时药物治疗的绩效指标根据指南预先设定,为所有患者系统收集,并纳入一个集中数据库。
688例患者(54.6%)出院时主要诊断为ST段抬高型心肌梗死(STEMI),491例(39%)为非ST段抬高型心肌梗死(NSTEMI),81例(6.4%)为不稳定型心绞痛。平均年龄为64岁,女性占21.3%。仅考虑原始处方率时,94.6%的患者出院时开具了血管紧张素转换酶抑制剂/血管紧张素II受体阻滞剂,但纳入未处方原因后,这一比例增至99.5%。对于他汀类药物,纳入未处方原因后,比例从98%增至98.6%;对于β受体阻滞剂,从82%增至93%。对于阿司匹林,比例从99.4%进一步增至100%,对于P2Y12抑制剂,从99.8%增至100%。
当纳入药物治疗未处方的原因时,我们发现出院时对ACS指南中药物处方的遵循度非常高。对于β受体阻滞剂,即使考虑了未处方原因,处方率仍未达到最佳水平。在一个致力于提高医疗质量以实现出院时100%处方率(除非有禁忌证)的时代,预先设定心血管预防性药物未处方的原因有助于识别出院时医疗质量方面仍存在的差距。
ClinicalTrials.gov NCT01000701