Estevez-Loureiro Rodrigo, Ghione Matteo, Kilickesmez Kadriye, Agudo Pilar, Lindsay Alistair, Di Mario Carlo
Royal Brompton Hospital, Sydney Street, London, Greater London SW3 6NP, UK.
Curr Cardiol Rev. 2014 May;10(2):120-6. doi: 10.2174/1573403x10666140331143731.
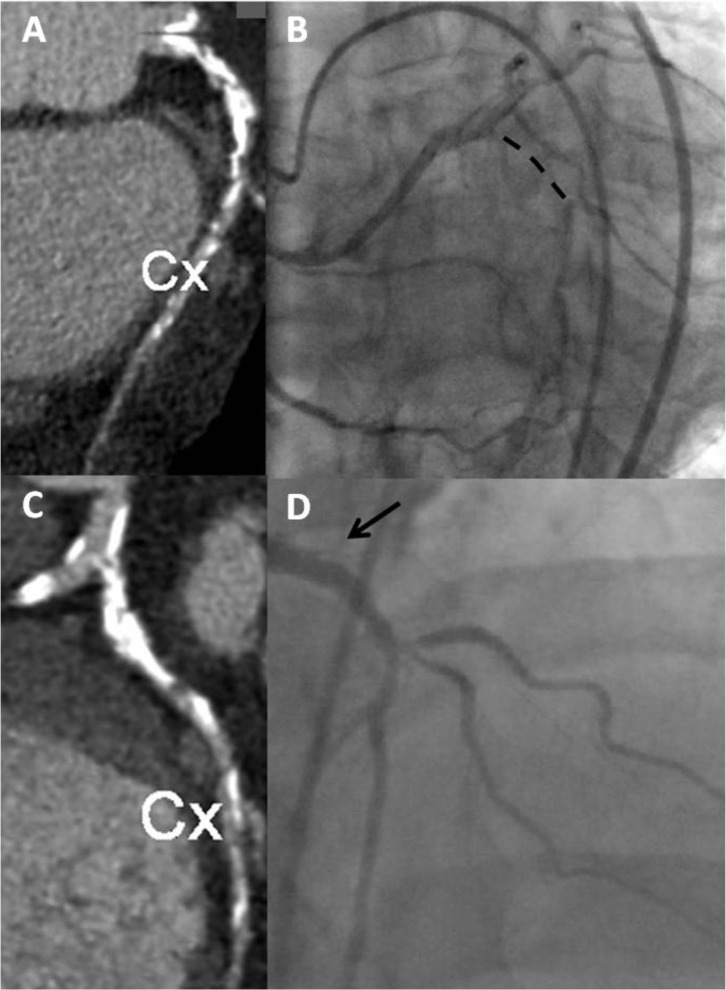
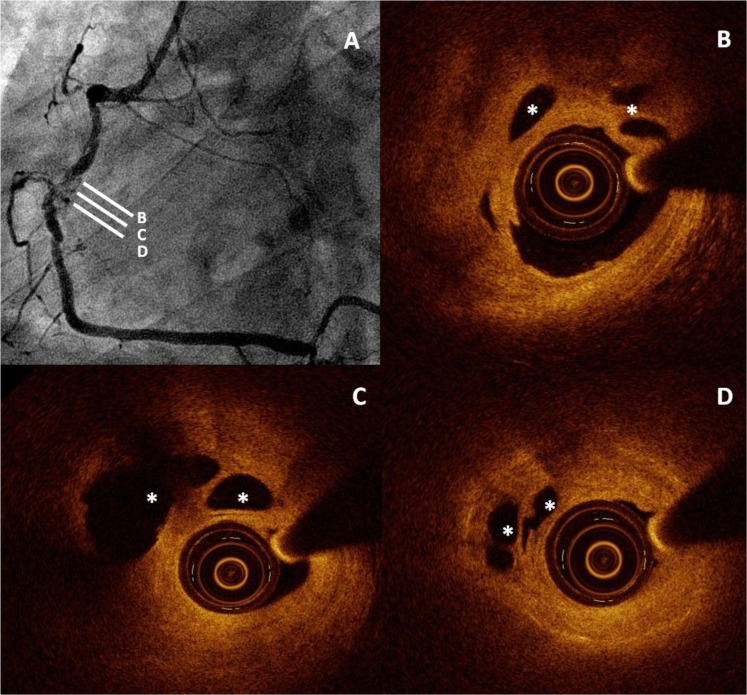
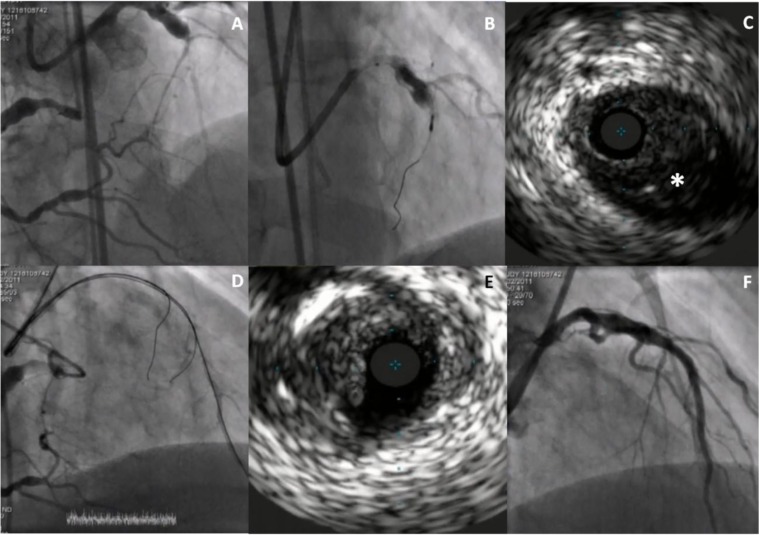
Non invasive coronary angiography with multislice computed tomography has exquisite sensitivity to detect calcium and even the faintest late contrast filling of the distal vessel. Calcium burden and occlusion length are still valuable markers of duration, complexity and success of the recanalisation procedure. The ability to visualise the vessel also in the occluded segment, especially if calcified, can also help the operator to understand where to pierce the proximal cap in stumpless occlusions and to predict unusual courses, especially in very tortuous arteries. Imaging side by side CT images and angiography during the recanalisation procedure is an established practice in many active CTO laboratories and algorithms for co-registration are designed to overcome the challenges of systo-diastolic and respiratory motion. Intravascular ultrasound is used in almost all cases by the experienced Japanese CTO operators but most of the times its main use is a better identification of the diseased segment after predilatation to ensure complete stent cover and appropriate stent expansion, an application similar to other complex non occlusive lesions. The specificity of IVUS during CTO recanalisation is the identification of the vessel path in stumpless occlusions and the guidance of wire reentry especially during reverse Controlled Retrograde Anterograde Tracking. Optical coherence tomography has limitations in the setting of CTO recanalisation because of the need of forceful contrast flushing to clear blood, contraindicated in the presence of anterograde dissections, and the limited penetration. The variability in the use of both non-invasive and invasive imaging during CTO recanalisation is immense, going from more than 90% in Japan to less than 20% in Europe and intermediate penetration in the USA. Probably the explanation is almost only in availability and cost because all countries see a progressive increase of use suggesting that these methods are becoming an established tool for guidance of CTO recanalisation.
多层螺旋计算机断层扫描的无创冠状动脉造影对检测钙化甚至远端血管最微弱的延迟造影剂充盈具有极高的敏感性。钙化负荷和闭塞长度仍然是再通手术持续时间、复杂性和成功与否的重要指标。在闭塞段可视化血管的能力,特别是在钙化情况下,也有助于术者了解在无残端闭塞时从何处穿刺近端帽,并预测异常走行,尤其是在非常迂曲的动脉中。在再通手术过程中同时观察CT图像和血管造影是许多活跃的慢性完全闭塞病变(CTO)实验室的既定做法,并且用于配准的算法旨在克服心脏收缩-舒张和呼吸运动带来的挑战。经验丰富的日本CTO术者在几乎所有病例中都使用血管内超声,但大多数情况下,其主要用途是在预扩张后更好地识别病变段,以确保支架完全覆盖并适当扩张,这一应用与其他复杂的非闭塞性病变类似。CTO再通期间血管内超声的独特之处在于识别无残端闭塞中的血管路径以及引导导丝重新进入,特别是在逆向控制性逆行内膜下寻径技术中。光学相干断层扫描在CTO再通的情况下存在局限性,因为需要强力冲洗造影剂以清除血液,在存在顺行夹层时是禁忌的,并且穿透深度有限。在CTO再通期间,无创和有创成像的使用差异极大,从日本的超过90%到欧洲的不到20%,美国则处于中间水平。可能的解释几乎完全在于可获得性和成本,因为所有国家的使用都在逐步增加,这表明这些方法正成为CTO再通指导的既定工具。