University Hospitals Case Medical Center, Case Western Reserve University, 10524 Euclid Ave., 12th Floor, Cleveland, OH, 44106, USA,
CNS Drugs. 2014 Jun;28(6):571-81. doi: 10.1007/s40263-014-0158-2.
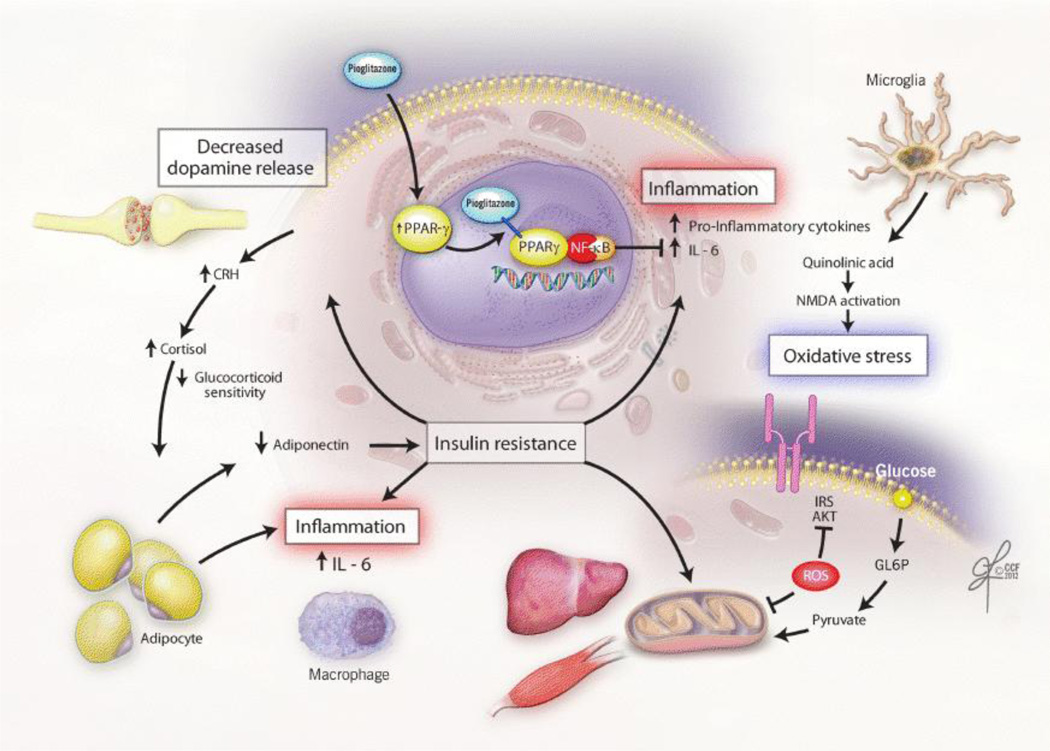
Insulin resistance and other cardio-metabolic risk factors predict increased risk of depression and decreased response to antidepressant and mood stabilizer treatments. This proof-of-concept study tested whether administration of an insulin-sensitizing peroxisome proliferator-activated receptor (PPAR)-γ agonist could reduce bipolar depression symptom severity. A secondary objective was to determine whether levels of highly sensitive C-reactive protein and interleukin (IL)-6 predicted treatment outcome.
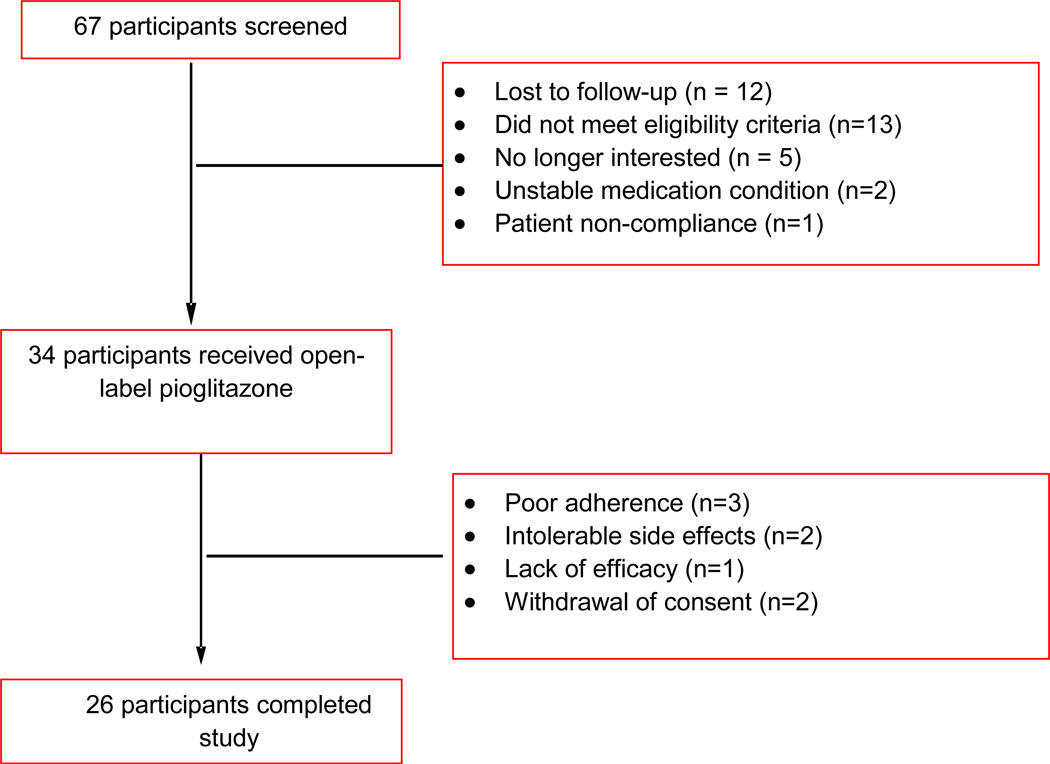
Patients (n = 34) with bipolar disorder (I, II, or not otherwise specified) and metabolic syndrome/insulin resistance who were currently depressed (Quick Inventory of Depressive Symptoms [QIDS] total score ≥11) despite an adequate trial of a mood stabilizer received open-label, adjunctive treatment with the PPAR-γ agonist pioglitazone (15-30 mg/day) for 8 weeks. The majority of participants (76 %, n = 26) were experiencing treatment-resistant bipolar depression, having already failed two mood stabilizers or the combination of a mood stabilizer and a conventional antidepressant.
Supporting an association between insulin sensitization and depression severity, pioglitazone treatment was associated with a decrease in the total Inventory of Depressive Symptomatology (IDS-C30) score from 38.7 ± 8.2 at baseline to 21.2 ± 9.2 at week 8 (p < 0.001). Self-reported depressive symptom severity and clinician-rated anxiety symptom severity significantly improved over 8 weeks as measured by the QIDS (p < 0.001) and Structured Interview Guide for the Hamilton Anxiety Scale (p < 0.001), respectively. Functional improvement also occurred as measured by the change in total score on the Sheehan Disability Scale (-17.9 ± 3.6; p < 0.001). Insulin sensitivity increased from baseline to week 8 as measured by the Insulin Sensitivity Index derived from an oral glucose tolerance test (0.98 ± 0.3; p < 0.001). Higher baseline levels of IL-6 were associated with greater decrease in depression severity (parameter estimate β = -3.89, standard error [SE] = 1.47, p = 0.015). A positive correlation was observed between improvement in IDS-C30 score and change in IL-6 (r = 0.44, p < 0.01).
Open-label administration of the PPAR-γ agonist pioglitazone was associated with improvement in depressive symptoms and reduced cardio-metabolic risk. Reduction in inflammation may represent a novel mechanism by which pioglitazone modulates mood. (ClinicalTrials.gov Identifier: NCT00835120).
胰岛素抵抗和其他心血管代谢风险因素可预测抑郁症风险增加和抗抑郁药及心境稳定剂治疗反应降低。这项验证概念的研究测试了给予胰岛素增敏过氧化物酶体增殖物激活受体(PPAR)-γ激动剂是否可以减轻双相抑郁的严重程度。次要目标是确定高敏 C 反应蛋白和白细胞介素(IL)-6 水平是否可以预测治疗结果。
患有双相障碍(I、II 或未特定)和代谢综合征/胰岛素抵抗的患者(无论是否符合),尽管已接受适当的心境稳定剂治疗,但仍处于抑郁状态(贝克抑郁自评量表[BDI]总分≥11),接受 PPAR-γ 激动剂吡格列酮(15-30mg/天)的开放标签辅助治疗,为期 8 周。大多数参与者(76%,n=26)患有治疗抵抗性双相抑郁,已经对两种心境稳定剂或心境稳定剂和传统抗抑郁药联合治疗无效。
支持胰岛素增敏与抑郁严重程度之间的关联,吡格列酮治疗与贝克抑郁自评量表(IDS-C30)总分从基线时的 38.7±8.2 降至第 8 周时的 21.2±9.2(p<0.001)相关。第 8 周时,贝克抑郁自评量表(p<0.001)和汉密尔顿焦虑量表结构访谈指南(p<0.001)分别自我报告的抑郁症状严重程度和临床医生评定的焦虑症状严重程度均显著改善。用 Sheehan 残疾量表(-17.9±3.6;p<0.001)总评分的变化也表明功能得到改善。用口服葡萄糖耐量试验得出的胰岛素敏感性指数(0.98±0.3;p<0.001)测量,胰岛素敏感性从基线到第 8 周增加。
PPAR-γ 激动剂吡格列酮的开放标签给药与抑郁症状改善和降低心血管代谢风险有关。炎症的减少可能代表吡格列酮调节情绪的新机制。(临床试验标识符:NCT00835120)。