Department of Clinical Sciences, Division of Oncology and Pathology, Lund University, Skåne University Hospital, Lund SE-221 85, Sweden.
Diagn Pathol. 2014 Apr 14;9:80. doi: 10.1186/1746-1596-9-80.
Variability in reported histopathology parameters in operated periampullary adenocarcinomas may affect the prognostic weight of the parameters. Standardized axial sectioning produces a higher incidence of involved margins and also seems to produce a lower relative incidence of pancreatic compared with distal bile duct origin and a higher incidence of involved lymph nodes, compared with non-standardized procedure. The aims of this study were to 1) assess how a previously not described standardized pathology procedure, with longitudinal sectioning along the distal bile duct, affects reported tumour origin, margin status and involved lymph nodes, compared with non-standardized procedure, 2) assess if re-evaluation of microscopic slides affects the prognostic value of margin status and 3) compare the results of this standardized procedure with reported results of other standardized and non-standardized procedures.
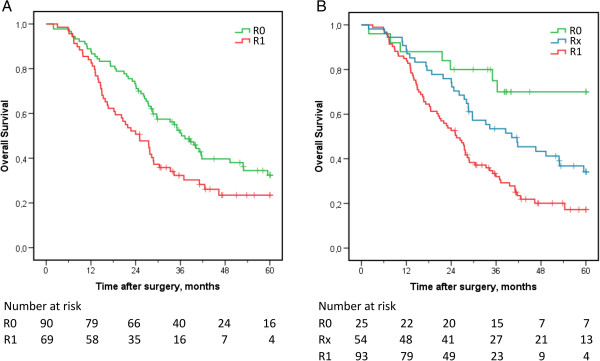
One hundred seventy-five consecutive pancreaticoduodenectomy specimens with primary adenocarcinomas, operated during 2001 - 2011 at the University hospitals of Lund and Malmö, Sweden, were re-evaluated histologically, and parameters relevant for classification and prognosis were assessed, with 1 mm as a threshold for involved or uninvolved margins. Follow-up lasted until 31 December 2013. Five-year overall survival (OS) and hazard ratios (HR) were calculated for the margin status stated in the original reports and margin status after re-evaluation.
Compared with non-standardized cases (n = 129), standardized cases (n = 46) had more involved lymph nodes in the specimens (median 3 vs 1), a higher fraction of distal bile duct origin (39% vs 21%) and a higher fraction of involved margins (74% vs 47%). The prognostic value of uninvolved margins increased by re-evaluation of slides (p < 0.001) and the adjusted HR for involved margins increased from 1.6 (95% CI 1.1 - 2.4) to 3.3 (95% CI 1.5 - 7.0). Uninvolved margins remained a significant predictor of OS in adjusted analysis.
Both the method of sectioning the specimen and the microscopic assessment affect prognostic pathology parameters significantly. The results of the herein described standardized method are similar to the results of other standardized procedures. The 1-mm threshold for involved margins in pancreaticoduodenectomies is relevant for OS, and margin status is an independent prognostic parameter.
The virtual slides for this article can be found here: http://www.diagnosticpathology.diagnomx.eu/vs/1056639379120615.
在接受手术的胰头十二指肠腺癌中,报告的组织病理学参数的变异性可能会影响这些参数的预后权重。标准化轴向切片会增加受累切缘的发生率,并且似乎会降低与非标准化程序相比,胰腺起源与远端胆管起源的相对发生率,并增加受累淋巴结的发生率。本研究的目的是:1)评估以前未描述的标准化病理学程序(沿远端胆管进行纵向切片)与非标准化程序相比,如何影响报告的肿瘤起源、切缘状态和受累淋巴结;2)评估显微镜载玻片的重新评估是否会影响切缘状态的预后价值;3)将此标准化程序的结果与其他标准化和非标准化程序的报告结果进行比较。
对 2001 年至 2011 年在瑞典隆德大学医院和马尔默大学医院接受手术的 175 例原发性腺癌胰十二指肠切除术标本进行了重新评估,对组织学相关的分类和预后参数进行了评估,以 1mm 为界限来判断受累或未受累的切缘。随访至 2013 年 12 月 31 日。计算原始报告中切缘状态和重新评估后的切缘状态的 5 年总生存率(OS)和风险比(HR)。
与非标准化病例(n=129)相比,标准化病例(n=46)标本中的受累淋巴结更多(中位数 3 比 1),远端胆管起源比例更高(39%比 21%),受累切缘比例更高(74%比 47%)。载玻片的重新评估增加了未受累切缘的预后价值(p<0.001),并且受累切缘的调整 HR 从 1.6(95%CI 1.1-2.4)增加到 3.3(95%CI 1.5-7.0)。调整分析后,未受累切缘仍然是 OS 的显著预测因素。
标本的切片方法和显微镜评估都会显著影响预后病理学参数。本文描述的标准化方法的结果与其他标准化程序的结果相似。在胰十二指肠切除术中,1mm 作为受累切缘的界限与 OS 相关,切缘状态是独立的预后参数。