Bizet Jorge, Cooper Chad J, Quansah Raphael, Rodriguez Emmanuel, Teleb Mohamed, Hernandez German T
Department of Internal Medicine, Texas Tech University Health Sciences Center, El Paso, TX, U.S.A.
Am J Case Rep. 2014 Apr 7;15:143-6. doi: 10.12659/AJCR.890179. eCollection 2014.
Female, 66 FINAL DIAGNOSIS: Chorea • hyperglycemia • Basal Ganglia Syndrome (C-H-BG) Symptoms: Hemibalism • hemichorea
Challenging differential diagnosis.
Hemichorea-hemiballism (HCHB) is a spectrum of involuntary, continuous non-patterned movement involving 1 side of the body. Possible causes of HCHB include hemorrhagic or ischemic stroke, neoplasm, systemic lupus erythematosus, HHNK, Wilson's disease, and thyrotoxicosis. This case illustrates the need to be aware of hyperglycemia as a cause of hemiballism/hemichorea, which is now referred to in the medical literature as C-H-BG (chorea, hyperglycemia, basal ganglia) syndrome.
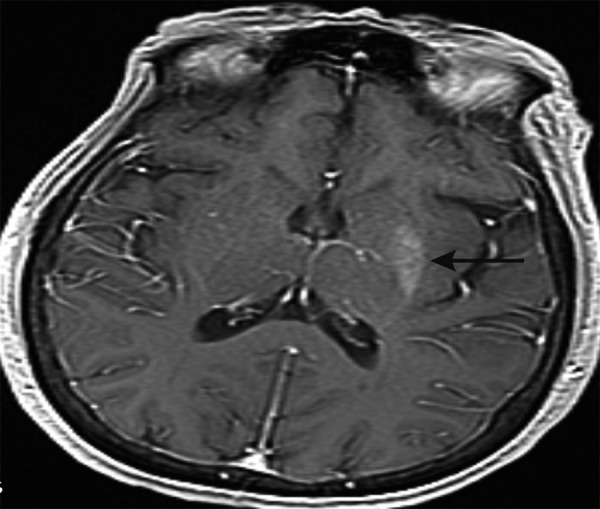
A 66-year-old Hispanic woman presented to our care with hemiballism/hemichorea of the right arm and leg of 1 week duration. She had been admitted 3 months prior with toxic metabolic encephalopathy secondary to hyperosmolar hyperglycemic non-ketotic syndrome with a blood glucose level of 984 mg/dL. Her blood glucose level was normal but hemoglobin A1C was 12.2%. A brain MRI revealed an asymmetric T1 hyperintensity of the left putamen. This specific finding was compatible with hyperglycemia-induced hemichorea hemiballism syndrome. The hemiballism/hemichorea slowly improved over the course of the hospitalization with strict glycemic control. At the 3-month follow-up visit she had no involuntary movements of her extremities, and she had well controlled blood glucose levels and a hemoglobin A1C of 9.0.
In a patient with normal glycemic levels but a history of uncontrolled diabetes, C-H-BG syndrome should be on the top of the differential list when the characteristic MRI findings of a hyperintensity in the basal ganglia are observed. This is a rare disease that deserves attention because it is reversible with correction of hyperglycemia. Thus, prompt recognition and treatment is essential to avoid adverse outcomes.
女性,66岁 最终诊断:舞蹈症 • 高血糖 • 基底节综合征(C-H-BG) 症状:偏身投掷症 • 偏身舞蹈症
具有挑战性的鉴别诊断
偏身舞蹈症-偏身投掷症(HCHB)是一种涉及身体一侧的不自主、持续且无规律的运动。HCHB的可能病因包括出血性或缺血性中风、肿瘤、系统性红斑狼疮、高渗高血糖非酮症综合征(HHNK)、威尔逊病和甲状腺毒症。该病例表明需要意识到高血糖是偏身投掷症/偏身舞蹈症的一个病因,在医学文献中现在将其称为C-H-BG(舞蹈症、高血糖、基底节)综合征。
一名66岁的西班牙裔女性因右臂和右腿偏身舞蹈症/偏身投掷症前来就诊,病程1周。她3个月前因高渗高血糖非酮症综合征继发的中毒性代谢性脑病入院,血糖水平为984 mg/dL。她的血糖水平正常,但糖化血红蛋白A1C为12.2%。脑部MRI显示左侧壳核不对称T1高信号。这一特定发现与高血糖诱导的偏身舞蹈症-偏身投掷症综合征相符。通过严格的血糖控制,偏身舞蹈症/偏身投掷症在住院期间逐渐改善。在3个月的随访中,她的四肢没有不自主运动,血糖水平得到良好控制,糖化血红蛋白A1C为9.0。
对于血糖水平正常但有糖尿病控制不佳病史的患者,当观察到基底节高信号这一特征性MRI表现时,C-H-BG综合征应列在鉴别诊断清单的首位。这是一种罕见疾病,值得关注因为它可通过纠正高血糖而逆转。因此,及时识别和治疗对于避免不良后果至关重要。