Brady Stefen, Squier Waney, Sewry Caroline, Hanna Michael, Hilton-Jones David, Holton Janice L
MRC Centre for Neuromuscular Diseases, UCL Institute of Neurology and National Hospital for Neurology and Neurosurgery, London, UK.
BMJ Open. 2014 Apr 28;4(4):e004552. doi: 10.1136/bmjopen-2013-004552.
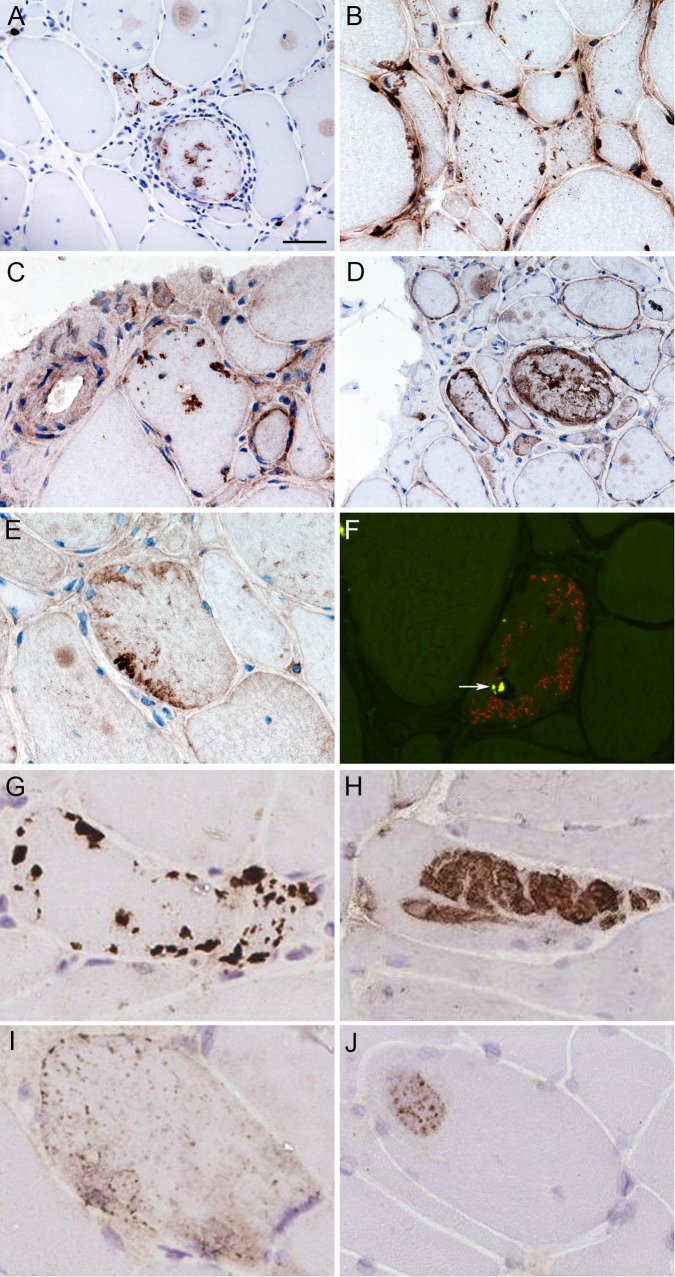
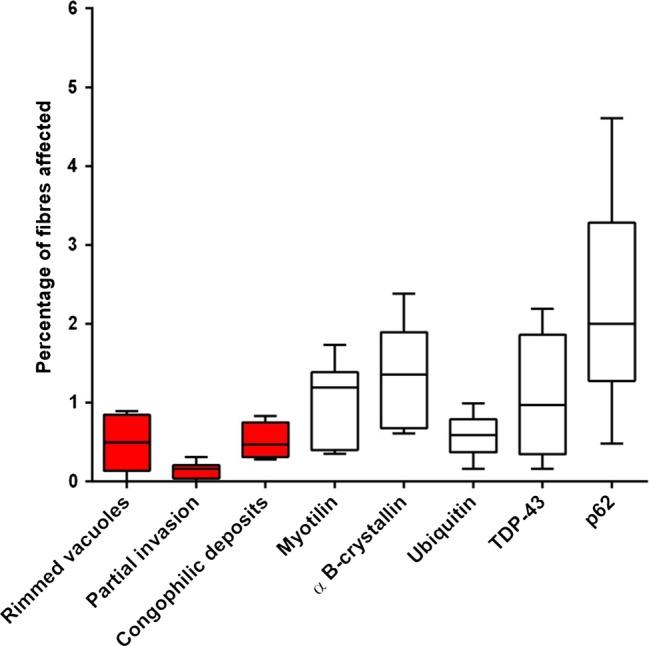
The current pathological diagnostic criteria for sporadic inclusion body myositis (IBM) lack sensitivity. Using immunohistochemical techniques abnormal protein aggregates have been identified in IBM, including some associated with neurodegenerative disorders. Our objective was to investigate the diagnostic utility of a number of markers of protein aggregates together with mitochondrial and inflammatory changes in IBM.
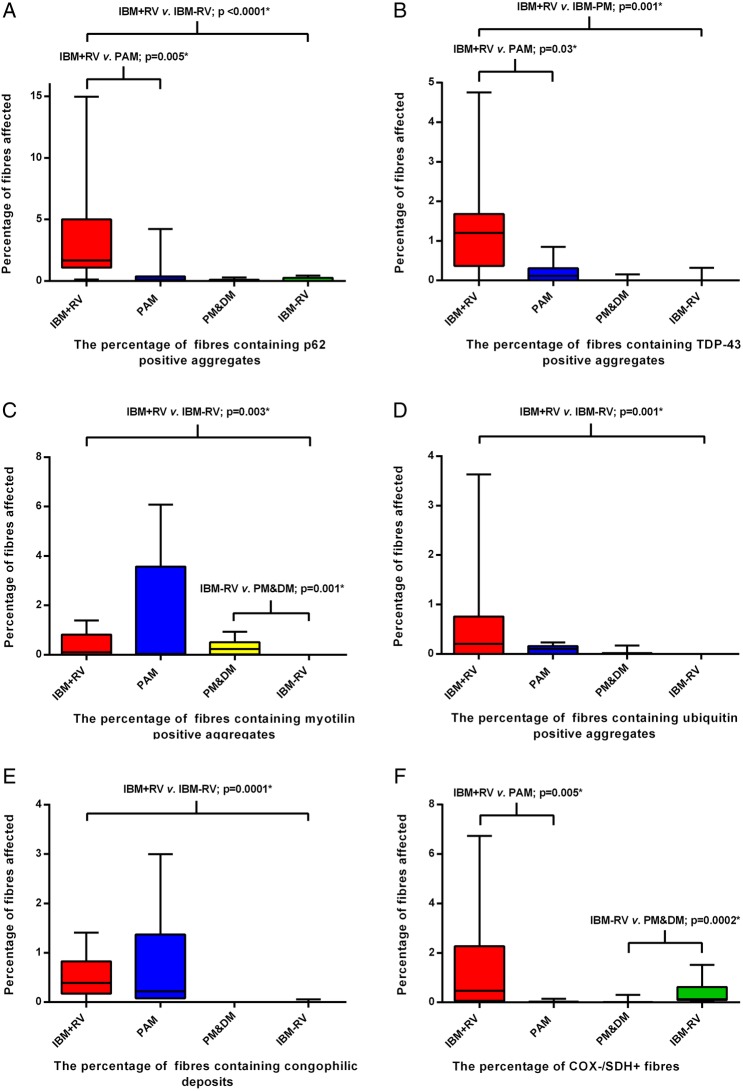
Retrospective cohort study. The sensitivity of pathological features was evaluated in cases of Griggs definite IBM. The diagnostic potential of the most reliable features was then assessed in clinically typical IBM with rimmed vacuoles (n=15), clinically typical IBM without rimmed vacuoles (n=9) and IBM mimics-protein accumulation myopathies containing rimmed vacuoles (n=7) and steroid-responsive inflammatory myopathies (n=11).
Specialist muscle services at the John Radcliffe Hospital, Oxford and the National Hospital for Neurology and Neurosurgery, London.
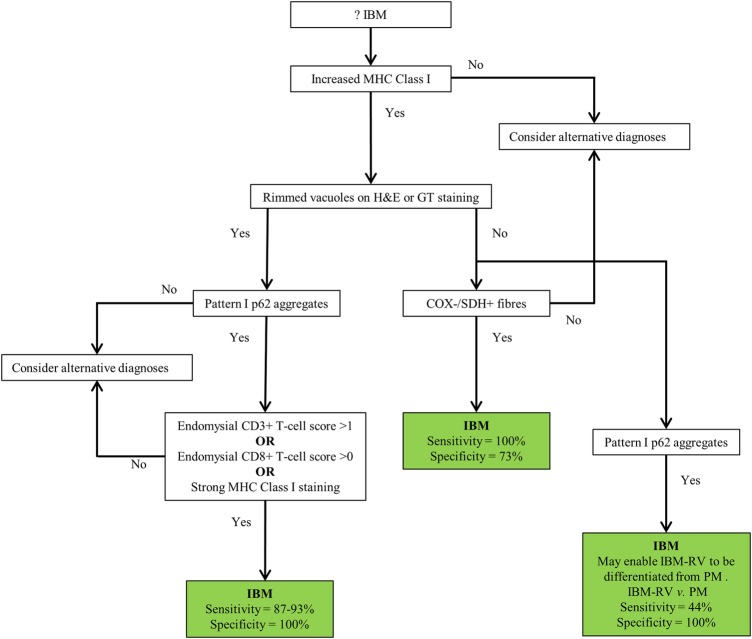
Individual pathological features, in isolation, lacked sensitivity and specificity. However, the morphology and distribution of p62 aggregates in IBM were characteristic and in a myopathy with rimmed vacuoles, the combination of characteristic p62 aggregates and increased sarcolemmal and internal major histocompatibility complex class I expression or endomysial T cells were diagnostic for IBM with a sensitivity of 93% and specificity of 100%. In an inflammatory myopathy lacking rimmed vacuoles, the presence of mitochondrial changes was 100% sensitive and 73% specific for IBM; characteristic p62 aggregates were specific (91%), but lacked sensitivity (44%).
We propose an easily applied diagnostic algorithm for the pathological diagnosis of IBM. Additionally our findings support the hypothesis that many of the pathological features considered typical of IBM develop later in the disease, explaining their poor sensitivity at disease presentation and emphasising the need for revised pathological criteria to supplement the clinical criteria in the diagnosis of IBM.
散发性包涵体肌炎(IBM)目前的病理诊断标准缺乏敏感性。利用免疫组化技术,已在IBM中鉴定出异常蛋白聚集体,包括一些与神经退行性疾病相关的蛋白聚集体。我们的目的是研究多种蛋白聚集体标志物以及IBM中线粒体和炎症变化的诊断效用。
回顾性队列研究。在Griggs确诊的IBM病例中评估病理特征的敏感性。然后在具有镶边空泡的临床典型IBM(n = 15)、无镶边空泡的临床典型IBM(n = 9)以及IBM模拟物——含有镶边空泡的蛋白积累性肌病(n = 7)和类固醇反应性炎性肌病(n = 11)中评估最可靠特征的诊断潜力。
牛津约翰·拉德克利夫医院和伦敦国立神经病学与神经外科医院的专科肌肉服务部门。
单独的个体病理特征缺乏敏感性和特异性。然而,IBM中p62聚集体的形态和分布具有特征性,在伴有镶边空泡的肌病中,特征性p62聚集体与肌膜和内部主要组织相容性复合体I类表达增加或肌内膜T细胞相结合对IBM具有诊断意义,敏感性为93%,特异性为100%。在缺乏镶边空泡的炎性肌病中,线粒体变化对IBM的敏感性为100%,特异性为73%;特征性p62聚集体具有特异性(91%),但缺乏敏感性(44%)。
我们提出了一种易于应用的IBM病理诊断算法。此外,我们的研究结果支持这样的假设,即许多被认为是IBM典型特征的病理特征在疾病后期才出现,这解释了它们在疾病表现时敏感性较差的原因,并强调需要修订病理标准以补充临床标准用于IBM的诊断。