O'Donnell Denis E, Maltais François, Porszasz Janos, Webb Katherine A, Albers Frank C, Deng Qiqi, Iqbal Ahmar, Paden Heather A, Casaburi Richard
Queen's University & Kingston General Hospital, Kingston, Ontario, Canada.
Centre de Recherche, Institut Universitaire de Cardiologie et de Pneumologie de Québec, Université Laval, Québec, Canada.
PLoS One. 2014 May 1;9(5):e96574. doi: 10.1371/journal.pone.0096574. eCollection 2014.
To have a better understanding of the mechanisms of exercise limitation in mild-to-moderate chronic obstructive pulmonary disease (COPD), we compared detailed respiratory physiology in patients with COPD and healthy age- and sex-matched controls.
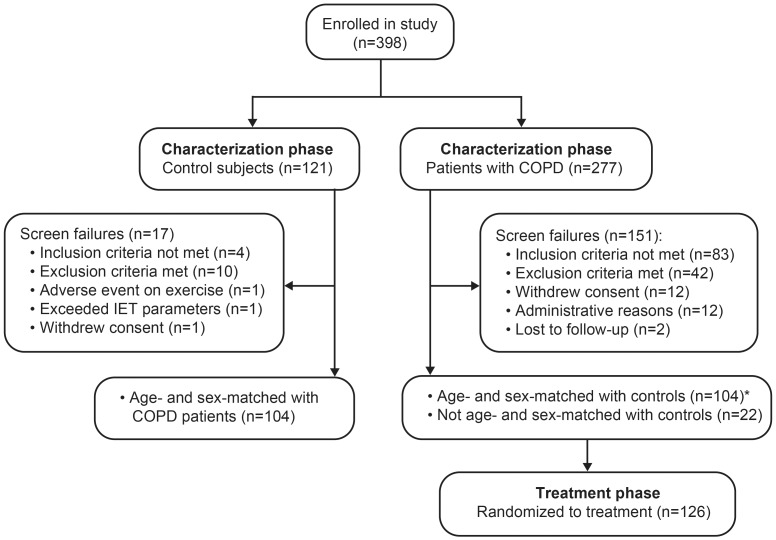
Data were collected during the pre-treatment, patient characterization phase of a multicenter, randomized, double-blind, crossover study. Patients with COPD met Global Initiative for Chronic Obstructive Lung Disease (GOLD) 1 or 2 spirometric criteria, were symptomatic, and had evidence of gas trapping during exercise. All participants completed pulmonary function and symptom-limited incremental treadmill exercise tests.
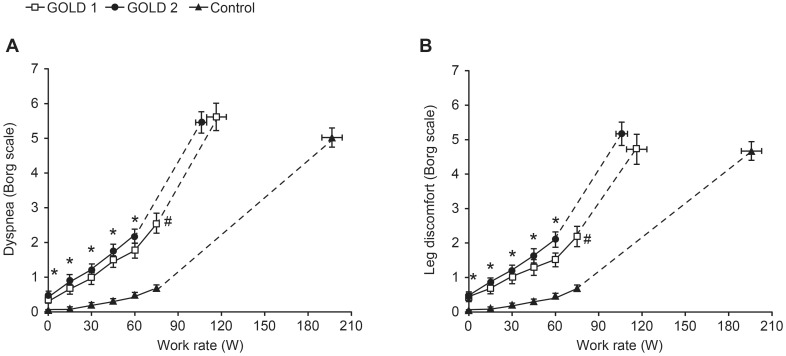
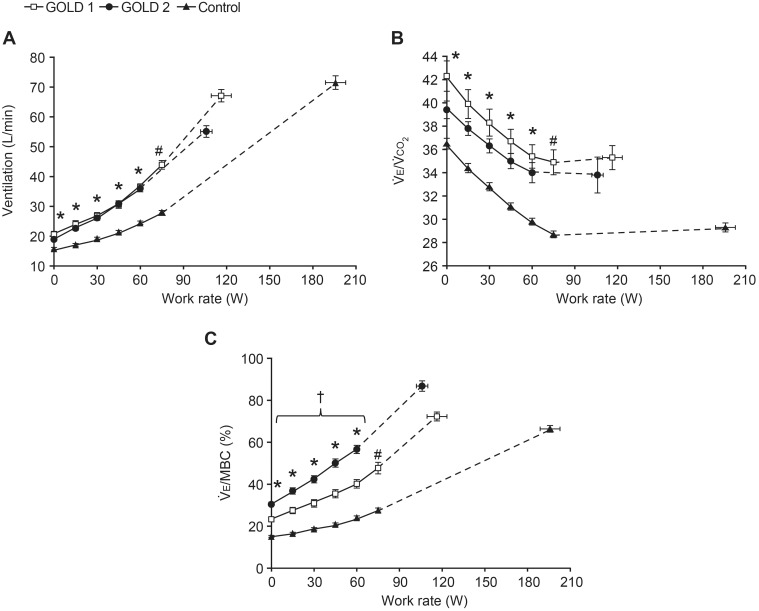
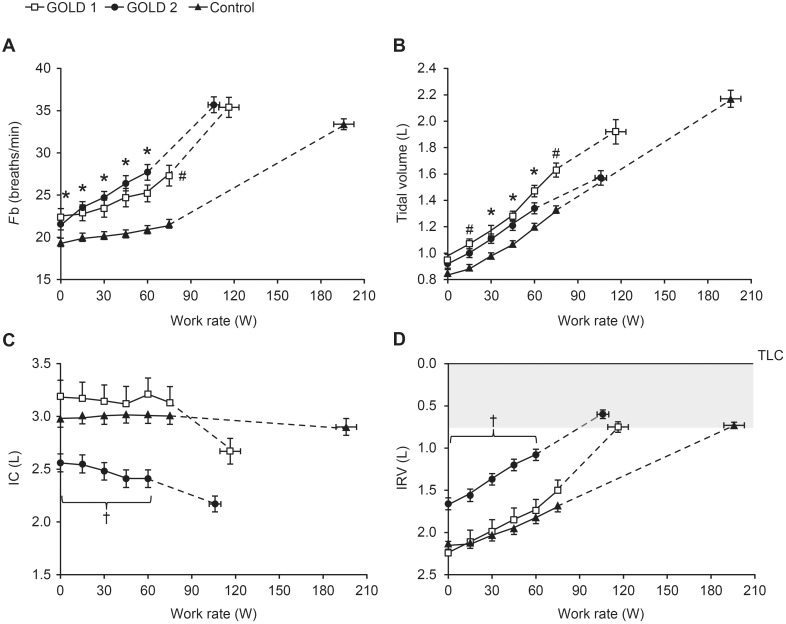
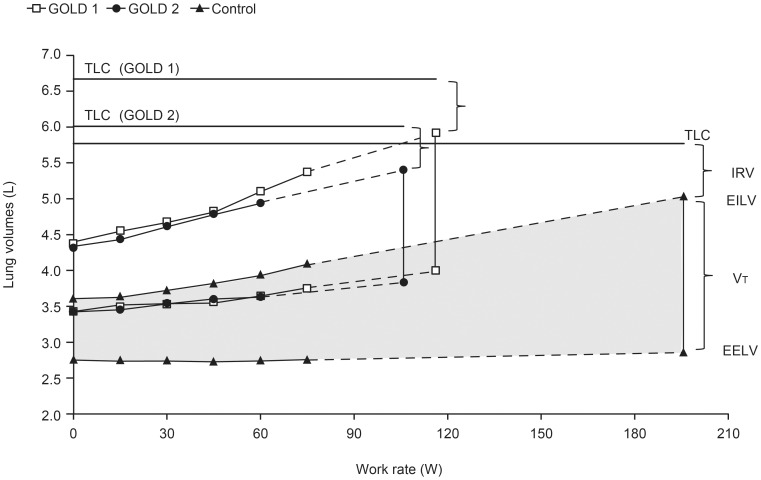
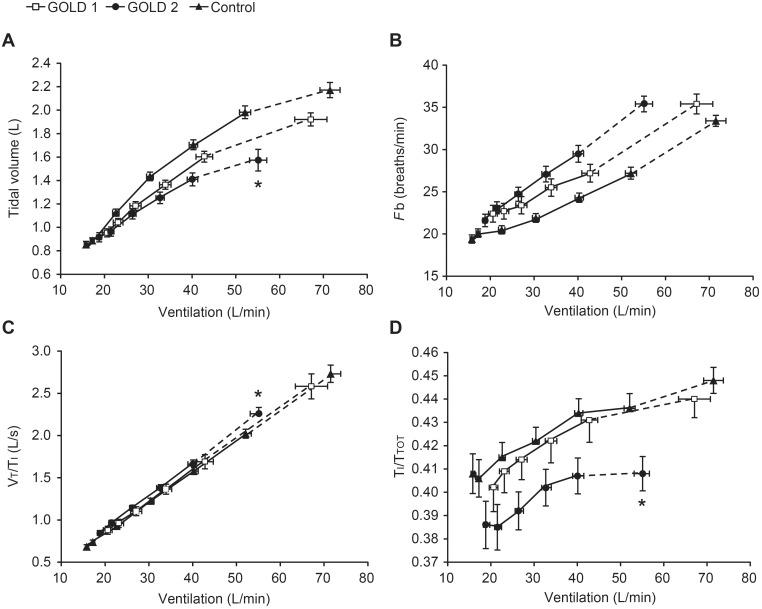
Chronic activity-related dyspnea measured by Baseline Dyspnea Index was similarly increased in patients with GOLD 1 (n = 41) and 2 (n = 63) COPD compared with controls (n = 104). Plethysmographic lung volumes were increased and lung diffusing capacity was decreased in both GOLD groups. Peak oxygen uptake and work rate were reduced in both GOLD groups compared with controls (p<0.001). Submaximal ventilation, dyspnea, and leg discomfort ratings were higher for a given work rate in both GOLD groups compared with controls. Resting inspiratory capacity, peak ventilation, and tidal volume were reduced in patients with GOLD 2 COPD compared with patients with GOLD 1 COPD and controls (p<0.001).
Lower exercise tolerance in patients with GOLD 1 and 2 COPD compared with controls was explained by greater mechanical abnormalities, greater ventilatory requirements, and increased subjective discomfort. Lower resting inspiratory capacity in patients with GOLD 2 COPD was associated with greater mechanical constraints and lower peak ventilation compared with patients with GOLD 1 COPD and controls.
ClinicalTrials.gov: NCT01072396.
为了更好地理解轻至中度慢性阻塞性肺疾病(COPD)运动受限的机制,我们比较了COPD患者与年龄和性别匹配的健康对照者的详细呼吸生理学特征。
数据收集于一项多中心、随机、双盲、交叉研究的预处理、患者特征描述阶段。COPD患者符合慢性阻塞性肺疾病全球倡议(GOLD)1级或2级肺量计标准,有症状,且运动时有气体潴留的证据。所有参与者均完成了肺功能和症状限制递增式平板运动试验。
与对照组(n = 104)相比,GOLD 1级(n = 41)和2级(n = 63)COPD患者中,通过基线呼吸困难指数测量的慢性活动相关呼吸困难程度同样增加。两个GOLD组的体积描记法肺容积均增加,肺扩散能力均降低。与对照组相比,两个GOLD组的峰值摄氧量和工作率均降低(p<0.001)。与对照组相比,两个GOLD组在给定工作率下的次最大通气量、呼吸困难和腿部不适评分更高。与GOLD 1级COPD患者和对照组相比,GOLD 2级COPD患者的静息吸气容量、峰值通气量和潮气量均降低(p<0.001)。
与对照组相比,GOLD 1级和2级COPD患者运动耐力较低的原因是机械异常更严重、通气需求更大以及主观不适增加。与GOLD 1级COPD患者和对照组相比,GOLD 2级COPD患者较低的静息吸气容量与更大的机械限制和更低的峰值通气量有关。
ClinicalTrials.gov:NCT01072396。