Xiang Nan, Wethington Holly, Onufrak Stephen, Belay Brook
University of Michigan Medical School, Ann Arbor, MI 48109, USA ; The CDC Experience Applied Epidemiology Fellowship, Scientific Education and Professional Development Program Office, Centers for Disease Control and Prevention, Atlanta, GA 30341, USA ; Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, 4770 Buford Hwy NE, MSK-26, Atlanta, GA 30341, USA.
Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention, 4770 Buford Hwy NE, MSK-26, Atlanta, GA 30341, USA.
Int J Pediatr. 2014;2014:987082. doi: 10.1155/2014/987082. Epub 2014 Mar 24.
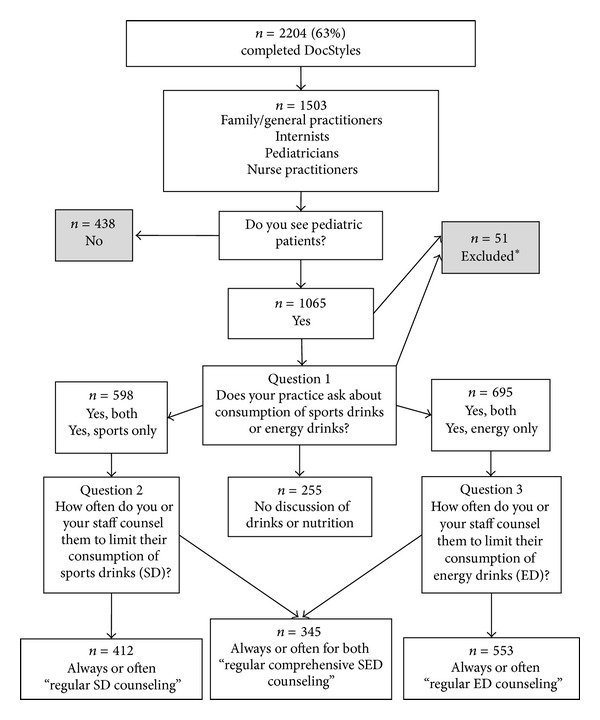
Objective. To examine the proportion of health care providers who counsel adolescent patients on sports and energy drink (SED) consumption and the association with provider characteristics. Methods. This is a cross-sectional analysis of a survey of providers who see patients ≤17 years old. The proportion providing regular counseling on sports drinks (SDs), energy drinks (EDs), or both was assessed. Chi-square analyses examined differences in counseling based on provider characteristics. Multivariate logistic regression calculated adjusted odds ratios (aOR) for characteristics independently associated with SED counseling. Results. Overall, 34% of health care providers regularly counseled on both SEDs, with 41% regularly counseling on SDs and 55% regularly counseling on EDs. On adjusted modeling regular SED counseling was associated with the female sex (aOR: 1.44 [95% CI: 1.07-1.93]), high fruit/vegetable intake (aOR: 2.05 [95% CI: 1.54-2.73]), family/general practitioners (aOR: 0.58 [95% CI: 0.41-0.82]) and internists (aOR: 0.37 [95% CI: 0.20-0.70]) versus pediatricians, and group versus individual practices (aOR: 0.59 [95% CI: 0.42-0.84]). Modeling for SD- and ED-specific counseling found similar associations with provider characteristics. Conclusion. The prevalence of regular SED counseling is low overall and varies. Provider education on the significance of SED counseling and consumption is important.
目的。探讨就运动和能量饮料(SED)消费向青少年患者提供咨询的医疗服务提供者的比例,以及与提供者特征的关联。方法。这是一项对诊治17岁及以下患者的提供者进行的调查的横断面分析。评估了就运动饮料(SD)、能量饮料(ED)或两者提供定期咨询的比例。卡方分析检验了基于提供者特征的咨询差异。多变量逻辑回归计算了与SED咨询独立相关特征的调整优势比(aOR)。结果。总体而言,34%的医疗服务提供者定期就SED两者提供咨询,41%定期就SD提供咨询,55%定期就ED提供咨询。在调整模型中,定期进行SED咨询与女性性别(aOR:1.44 [95%CI:1.07 - 1.93])、高水果/蔬菜摄入量(aOR:2.05 [95%CI:1.54 - 2.73])、家庭/全科医生(aOR:0.58 [95%CI:0.41 - 0.82])和内科医生(aOR:0.37 [95%CI:0.20 - 0.70])(与儿科医生相比)以及团体执业与个体执业(aOR:0.59 [95%CI:0.42 - 0.84])相关。针对SD和ED特定咨询的模型发现与提供者特征有类似关联。结论。总体而言,定期进行SED咨询的患病率较低且存在差异。对提供者进行关于SED咨询和消费重要性的教育很重要。