Abdelrahman Tamer, Hughes Joseph, Main Janice, McLauchlan John, Thursz Mark, Thomson Emma
MRC-University of Glasgow Centre for Virus Research, Glasgow, UK.
Hepatology. 2015 Jan;61(1):88-97. doi: 10.1002/hep.27192. Epub 2014 Jul 30.
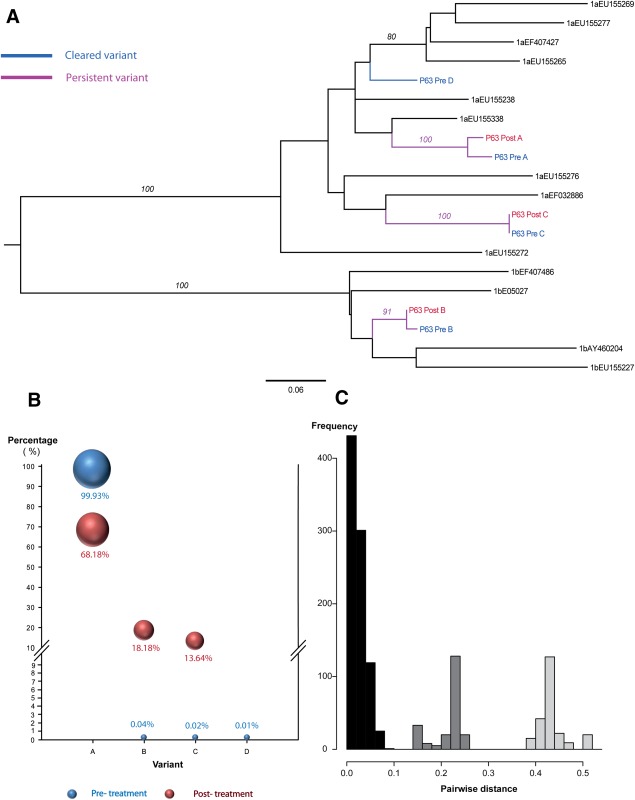
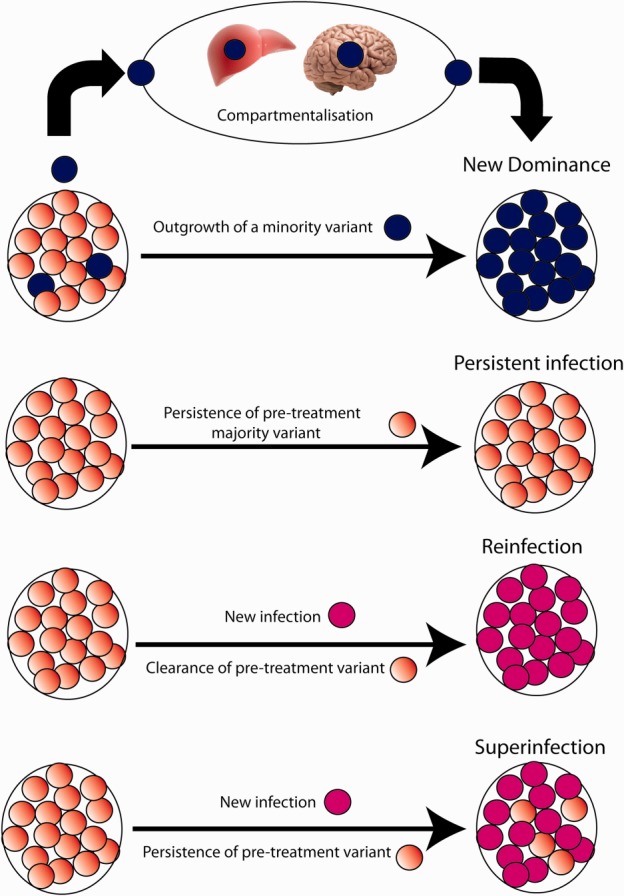
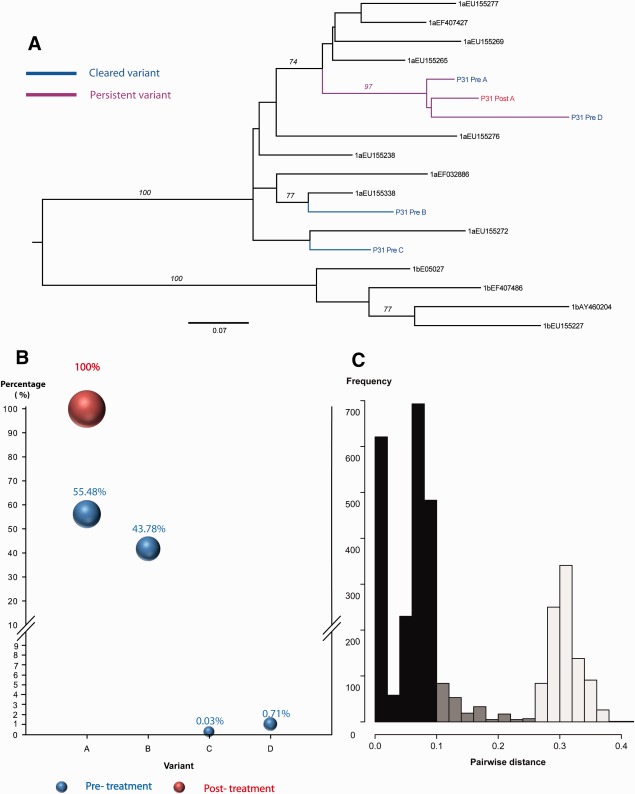
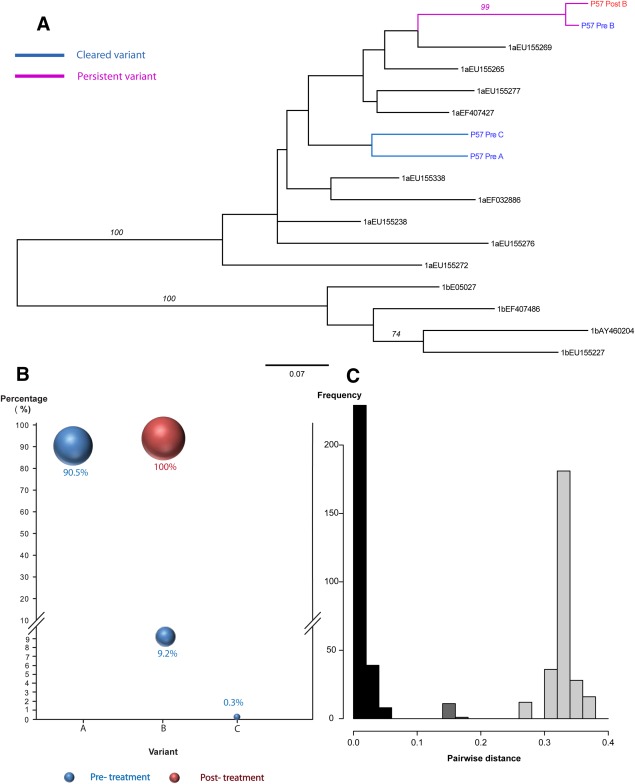
High rates of sexually transmitted infection and reinfection with hepatitis C virus (HCV) have recently been reported in human immunodeficiency virus (HIV)-infected men who have sex with men and reinfection has also been described in monoinfected injecting drug users. The diagnosis of reinfection has traditionally been based on direct Sanger sequencing of samples pre- and posttreatment, but not on more sensitive deep sequencing techniques. We studied viral quasispecies dynamics in patients who failed standard of care therapy in a high-risk HIV-infected cohort of patients with early HCV infection to determine whether treatment failure was associated with reinfection or recrudescence of preexisting infection. Paired sequences (pre- and posttreatment) were analyzed. The HCV E2 hypervariable region-1 was amplified using nested reverse-transcription polymerase chain reaction (RT-PCR) with indexed genotype-specific primers and the same products were sequenced using both Sanger and 454 pyrosequencing approaches. Of 99 HIV-infected patients with acute HCV treated with 24-48 weeks of pegylated interferon alpha and ribavirin, 15 failed to achieve a sustained virological response (six relapsed, six had a null response, and three had a partial response). Using direct sequencing, 10/15 patients (66%) had evidence of a previously undetected strain posttreatment; in many studies, this is interpreted as reinfection. However, pyrosequencing revealed that 15/15 (100%) of patients had evidence of persisting infection; 6/15 (40%) patients had evidence of a previously undetected variant present in the posttreatment sample in addition to a variant that was detected at baseline. This could represent superinfection or a limitation of the sensitivity of pyrosequencing.
In this high-risk group, the emergence of new viral strains following treatment failure is most commonly associated with emerging dominance of preexisting minority variants rather than reinfection. Superinfection may occur in this cohort but reinfection is overestimated by Sanger sequencing.
最近有报道称,在感染人类免疫缺陷病毒(HIV)的男同性恋者中,性传播感染和丙型肝炎病毒(HCV)再感染的发生率很高,并且在单纯感染的注射吸毒者中也有再感染的描述。传统上,再感染的诊断是基于治疗前后样本的直接桑格测序,而不是更敏感的深度测序技术。我们研究了在早期HCV感染的高危HIV感染队列中,未达到标准治疗方案的患者的病毒准种动态,以确定治疗失败是否与再感染或既往感染的复发有关。分析了配对序列(治疗前和治疗后)。使用带有索引的基因型特异性引物,通过巢式逆转录聚合酶链反应(RT-PCR)扩增HCV E2高变区-1,并使用桑格测序和454焦磷酸测序方法对相同产物进行测序。在99例接受24-48周聚乙二醇化干扰素α和利巴韦林治疗的急性HCV感染的HIV感染患者中,15例未实现持续病毒学应答(6例复发,6例无应答,3例部分应答)。使用直接测序,10/15例患者(66%)在治疗后有先前未检测到的毒株的证据;在许多研究中,这被解释为再感染。然而,焦磷酸测序显示,15/15例患者(100%)有持续感染的证据;6/15例患者(40%)除了在基线时检测到的变异体外,在治疗后样本中还有先前未检测到的变异体的证据。这可能代表了重叠感染或焦磷酸测序敏感性的局限性。
在这个高危群体中,治疗失败后新病毒株的出现最常见的是与既往少数变异体的优势出现有关,而不是再感染。该队列中可能发生重叠感染,但桑格测序高估了再感染的情况。