Brunner Elizabeth, Tohen Mauricio, Osuntokun Olawale, Landry John, Thase Michael E
Eli Lilly and Company, Indianapolis, IN, USA.
Department of Psychiatry, Health Sciences Center, University of New Mexico, Albuquerque, NM, USA.
Neuropsychopharmacology. 2014 Oct;39(11):2549-59. doi: 10.1038/npp.2014.101. Epub 2014 May 7.
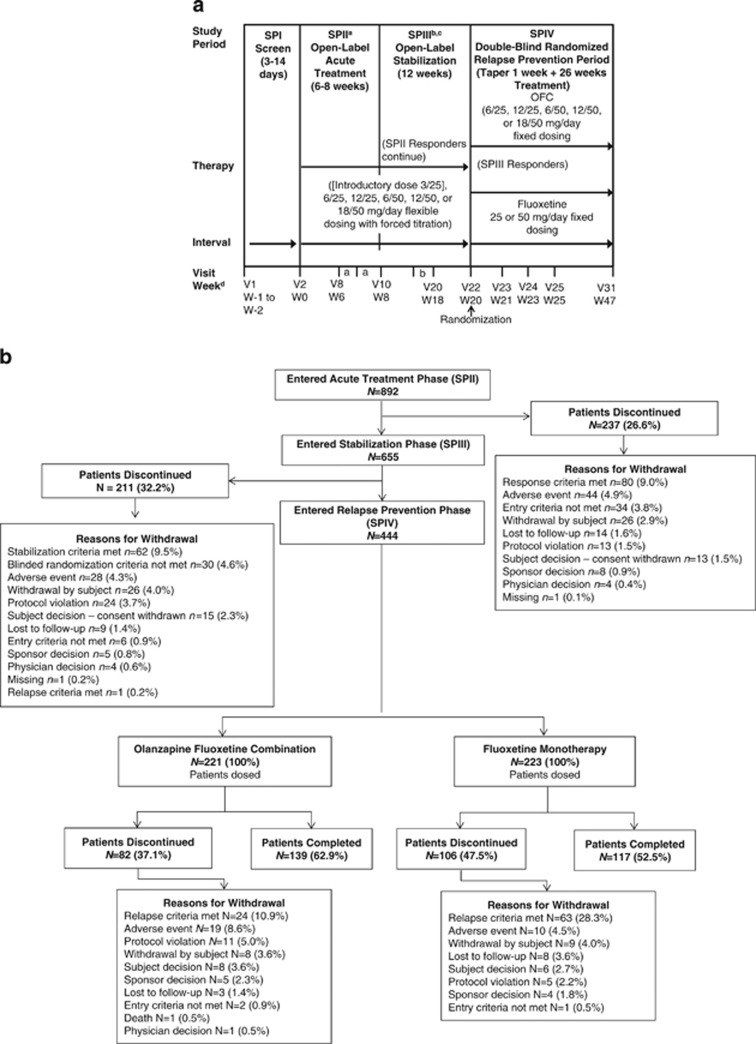
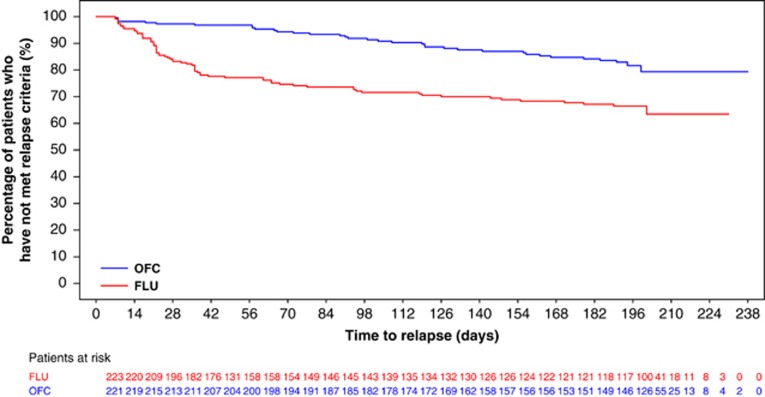
This study assessed prevention of relapse in patients with treatment-resistant depression (TRD) taking olanzapine/fluoxetine combination (OFC). Patients with major depressive disorder (MDD) who failed to satisfactorily respond to ≥ 2 different antidepressants for ≥ 6 weeks within the current MDD episode were acutely treated for 6-8 weeks, followed by stabilization (12 weeks) on OFC. Those who remained stable were randomized to OFC or fluoxetine for up to 27 weeks. Time-to-relapse was the primary efficacy outcome defined as 50% increase in Montgomery-Åsberg Depression Rating Scale score with Clinical Global Impressions-Severity of Depression score of ≥ 4; hospitalization for depression or suicidality; or discontinuation for lack of efficacy or worsening of depression or suicidality. A total of 444 patients were randomized 1:1 to OFC (N=221) or fluoxetine (N=223). Time-to-relapse was significantly longer in OFC-treated patients compared with fluoxetine-treated patients (p<0.001). Treatment-emergent weight gain and some mean and categorical fasting metabolic changes were significantly greater in OFC-treated patients. Clinically significant weight gain (≥ 7%) was observed in 55.7% of patients who remained on OFC throughout the study, including the relapse-prevention phase (up to 47 weeks). There were no significant differences between patients treated with OFC and fluoxetine in extrapyramidal symptoms or serious adverse events. We believe this is the first controlled relapse-prevention study in subjects with TRD that supports continued use of a second-generation antipsychotic beyond stabilization. A thorough assessment of benefits and risks (in particular metabolic changes) associated with continuing treatment with OFC or fluoxetine must be done based on individual patient needs.
本研究评估了服用奥氮平/氟西汀组合制剂(OFC)的难治性抑郁症(TRD)患者的复发预防情况。在当前重度抑郁发作期间,对≥2种不同抗抑郁药治疗≥6周仍未获得满意疗效的重度抑郁症(MDD)患者进行6 - 8周的急性治疗,随后用OFC进行12周的病情稳定治疗。病情保持稳定的患者被随机分为接受OFC或氟西汀治疗长达27周。复发时间是主要疗效指标,定义为蒙哥马利 - 奥斯伯格抑郁量表评分增加50%且临床总体印象 - 抑郁严重程度评分≥4;因抑郁或自杀倾向住院;或因疗效不佳、抑郁或自杀倾向恶化而停药。总共444例患者按1:1随机分为OFC组(N = 221)或氟西汀组(N = 223)。与氟西汀治疗的患者相比,OFC治疗的患者复发时间显著更长(p<0.001)。OFC治疗的患者出现的治疗中体重增加以及一些平均和分类的空腹代谢变化显著更大。在整个研究(包括复发预防阶段,长达47周)中持续使用OFC的患者中,55.7%出现了具有临床意义的体重增加(≥7%)。在锥体外系症状或严重不良事件方面,接受OFC和氟西汀治疗的患者之间没有显著差异。我们认为这是第一项针对TRD患者的对照复发预防研究,支持在病情稳定后继续使用第二代抗精神病药物。必须根据个体患者的需求,对继续使用OFC或氟西汀治疗相关的益处和风险(特别是代谢变化)进行全面评估。