Goyal Mayank, Almekhlafi Mohammed A, Fan Liqiong, Menon Bijoy K, Demchuk Andrew M, Yeatts Sharon D, Hill Michael D, Tomsick Thomas, Khatri Pooja, Zaidat Osama O, Jauch Edward C, Eesa Muneer, Jovin Tudor G, Broderick Joseph P
Departments of Radiology and Clinical Neurosciences, Calgary Stroke Program, University of Calgary, Calgary, Alberta, Canada (M.G., M.A.A., B.K.M., A.M.D., M.D.H., M.E.); Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia (M.A.A.); Department of Public Health Sciences, Medical University of South Carolina, Charleston (L.F., S.D.Y.); Departments of Neurology and Radiology, University of Cincinnati, Cincinnati, OH (T.T., P.K., J.P.B.); Department of Radiology, Medical College of Wisconsin, Milwaukee (O.O.Z.); Division of Emergency Medicine, Medical University of South Carolina, Charleston (E.C.J.); and Stroke Institute, University of Pittsburgh Medical Center, Pittsburgh, PA (T.G.J.).
Circulation. 2014 Jul 15;130(3):265-72. doi: 10.1161/CIRCULATIONAHA.113.007826. Epub 2014 May 9.
Meaningful delays occurred in the Interventional Management of Stroke (IMS) III trial. Analysis of the work flow will identify factors contributing to the in-hospital delays.
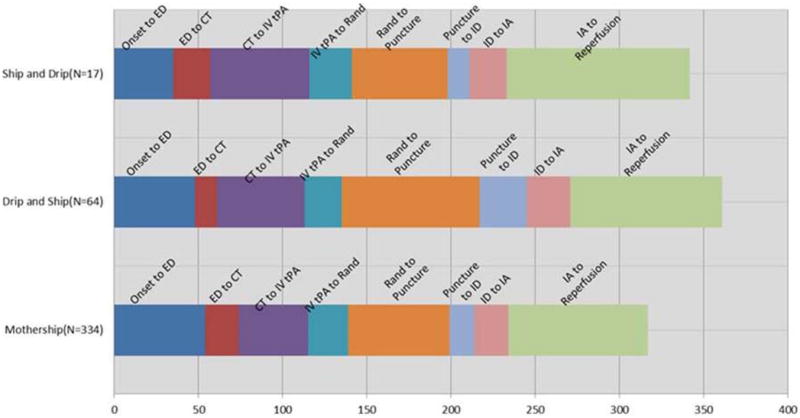
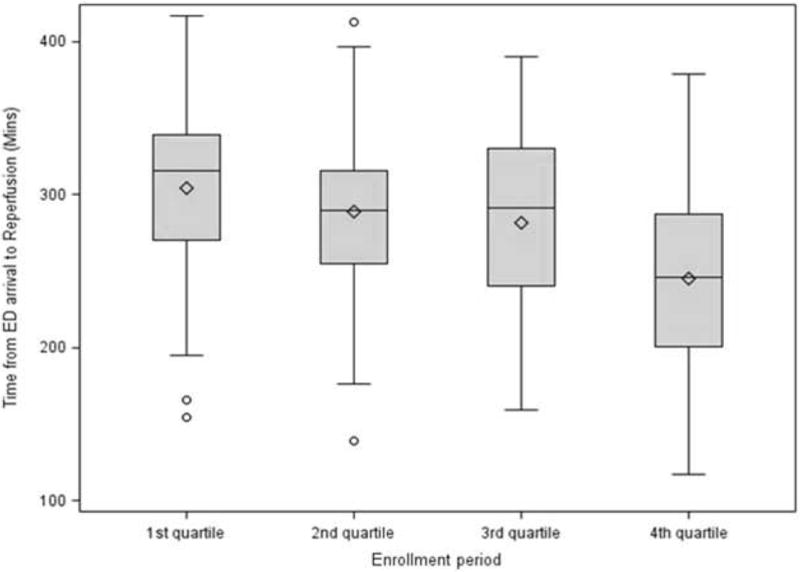
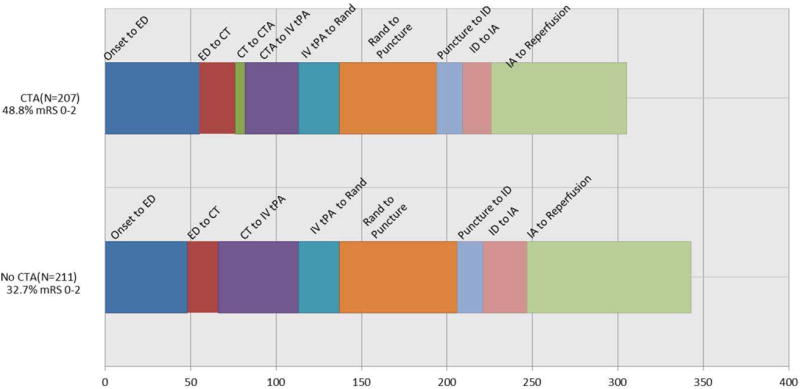
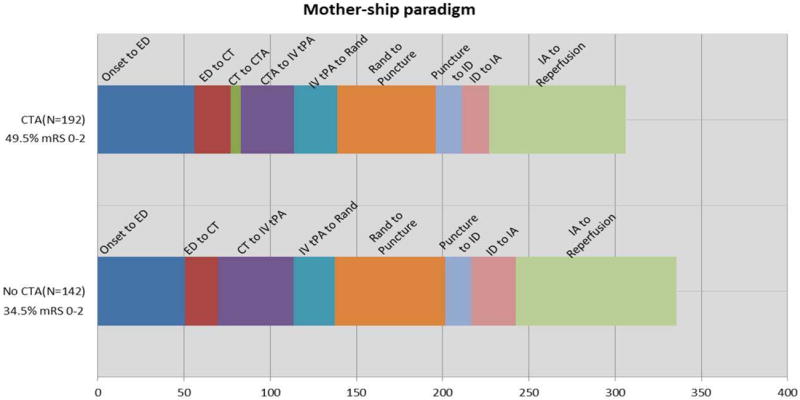
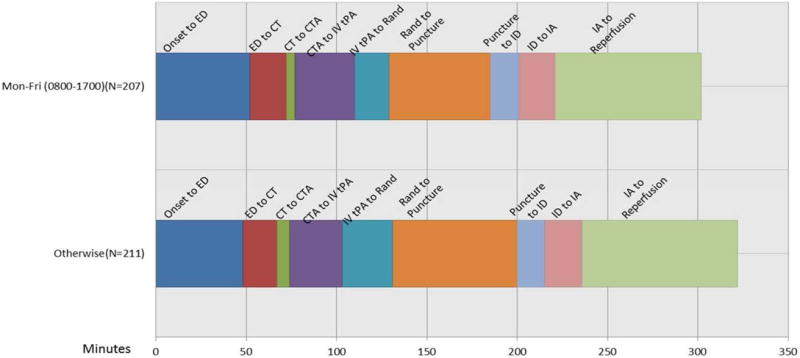
In the endovascular arm of the IMS III trial, the following time intervals were calculated: stroke onset to emergency department arrival; emergency department to computed tomography (CT); CT to intravenous tissue plasminogen activator start; intravenous tissue plasminogen activator start to randomization; randomization to groin puncture; groin puncture to thrombus identification; thrombus identification to start of endovascular therapy; and start of endovascular therapy to reperfusion. The effects of enrollment time, CT angiography use, interhospital transfers, and intubation on work flow were evaluated. Delays occurred notably in the time intervals from intravenous tissue plasminogen activator initiation to groin puncture (median 84 minutes) and start of endovascular therapy to reperfusion (median 85 minutes). The CT to groin puncture time was significantly shorter during working hours than after. Times from emergency department to reperfusion and groin puncture to reperfusion decreased over the trial period. Patients with CT angiography had shorter emergency department to reperfusion and onset to reperfusion times. Transfer of patients resulted in a longer onset to reperfusion time compared with those treated in the same center. Age, sex, National Institutes of Health Stroke Scale score, and intubation did not affect delays.
Important delays were identified before reperfusion in the IMS III trial. Delays decreased as the trial progressed. Use of CT angiography and endovascular treatment in the same center were associated with time savings. These data may help in optimizing work flow in current and future endovascular trials.
http://www.clinicaltrials.gov. Unique identifier: NCT00359424.
在卒中介入管理(IMS)III试验中出现了显著的延误。对工作流程进行分析将识别导致院内延误的因素。
在IMS III试验的血管内治疗组,计算了以下时间间隔:卒中发作至急诊科就诊;急诊科至计算机断层扫描(CT);CT至静脉注射组织型纤溶酶原激活剂开始;静脉注射组织型纤溶酶原激活剂开始至随机分组;随机分组至腹股沟穿刺;腹股沟穿刺至血栓识别;血栓识别至血管内治疗开始;以及血管内治疗开始至再灌注。评估了入组时间、CT血管造影的使用、院间转运和插管对工作流程的影响。在从静脉注射组织型纤溶酶原激活剂开始至腹股沟穿刺(中位数84分钟)以及血管内治疗开始至再灌注(中位数85分钟)的时间间隔中出现了明显延误。工作时间内CT至腹股沟穿刺的时间明显短于工作时间后。在试验期间,从急诊科至再灌注以及从腹股沟穿刺至再灌注的时间缩短。接受CT血管造影的患者从急诊科至再灌注以及从发作至再灌注的时间较短。与在同一中心接受治疗的患者相比,患者转运导致从发作至再灌注的时间更长。年龄、性别、美国国立卫生研究院卒中量表评分和插管均未影响延误情况。
在IMS III试验中,在再灌注前发现了重要延误。随着试验进展,延误减少。在同一中心使用CT血管造影和血管内治疗可节省时间。这些数据可能有助于优化当前及未来血管内试验的工作流程。