Leppin Aaron L, Gionfriddo Michael R, Kessler Maya, Brito Juan Pablo, Mair Frances S, Gallacher Katie, Wang Zhen, Erwin Patricia J, Sylvester Tanya, Boehmer Kasey, Ting Henry H, Murad M Hassan, Shippee Nathan D, Montori Victor M
Knowledge and Evaluation Research Unit, Mayo Clinic, Rochester, Minnesota.
Knowledge and Evaluation Research Unit, Mayo Clinic, Rochester, Minnesota2Mayo Graduate School, Mayo Clinic, Rochester, Minnesota.
JAMA Intern Med. 2014 Jul;174(7):1095-107. doi: 10.1001/jamainternmed.2014.1608.
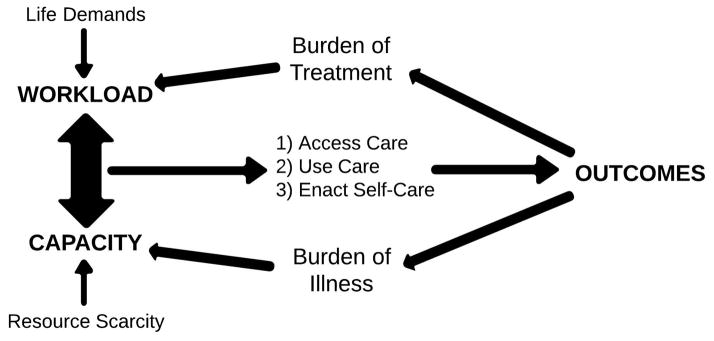
Reducing early (<30 days) hospital readmissions is a policy priority aimed at improving health care quality. The cumulative complexity model conceptualizes patient context. It predicts that highly supportive discharge interventions will enhance patient capacity to enact burdensome self-care and avoid readmissions.
To synthesize the evidence of the efficacy of interventions to reduce early hospital readmissions and identify intervention features--including their impact on treatment burden and on patients' capacity to enact postdischarge self-care--that might explain their varying effects.
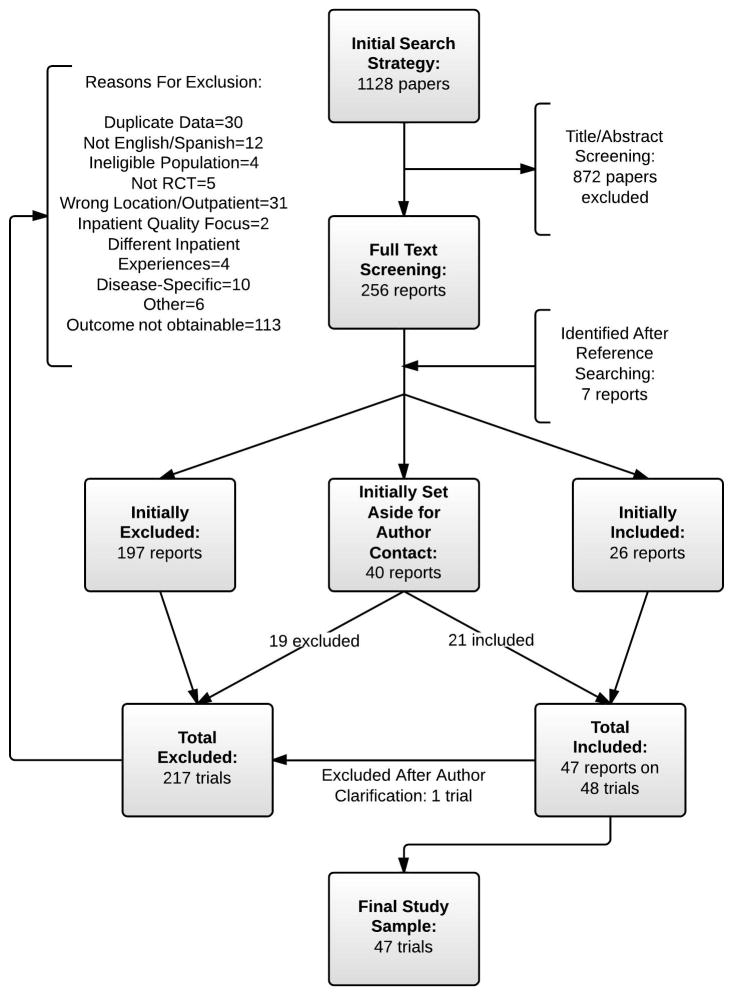
We searched PubMed, Ovid MEDLINE, Ovid EMBASE, EBSCO CINAHL, and Scopus (1990 until April 1, 2013), contacted experts, and reviewed bibliographies.
Randomized trials that assessed the effect of interventions on all-cause or unplanned readmissions within 30 days of discharge in adult patients hospitalized for a medical or surgical cause for more than 24 hours and discharged to home.
Reviewer pairs extracted trial characteristics and used an activity-based coding strategy to characterize the interventions; fidelity was confirmed with authors. Blinded to trial outcomes, reviewers noted the extent to which interventions placed additional work on patients after discharge or supported their capacity for self-care in accordance with the cumulative complexity model.
Relative risk of all-cause or unplanned readmission with or without out-of-hospital deaths at 30 days postdischarge.
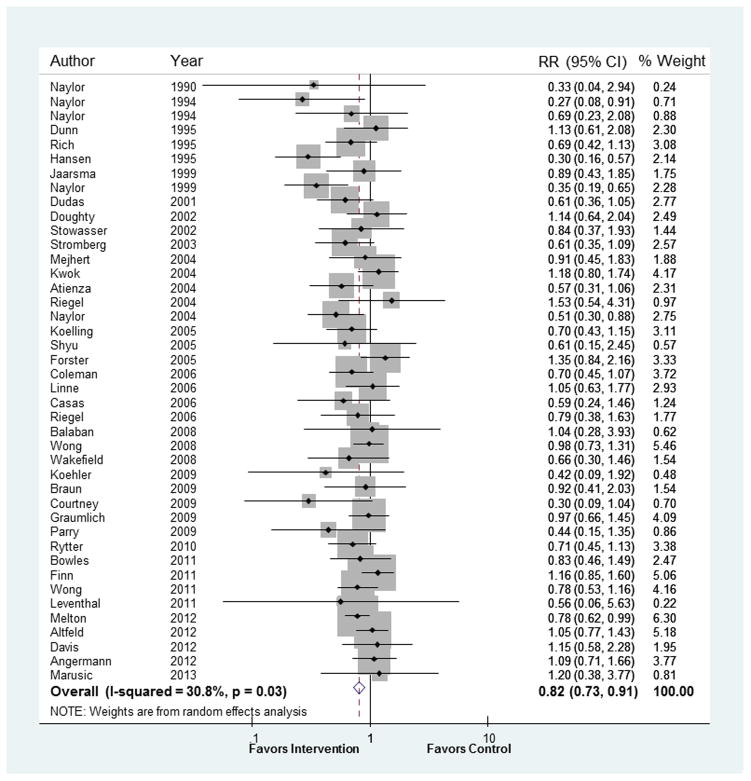
In 42 trials, the tested interventions prevented early readmissions (pooled random-effects relative risk, 0.82 [95% CI, 0.73-0.91]; P < .001; I² = 31%), a finding that was consistent across patient subgroups. Trials published before 2002 reported interventions that were 1.6 times more effective than those tested later (interaction P = .01). In exploratory subgroup analyses, interventions with many components (interaction P = .001), involving more individuals in care delivery (interaction P = .05), and supporting patient capacity for self-care (interaction P = .04) were 1.4, 1.3, and 1.3 times more effective than other interventions, respectively. A post hoc regression model showed incremental value in providing comprehensive, postdischarge support to patients and caregivers.
Tested interventions are effective at reducing readmissions, but more effective interventions are complex and support patient capacity for self-care. Interventions tested more recently are less effective.
降低早期(<30天)医院再入院率是旨在提高医疗质量的一项政策重点。累积复杂性模型将患者背景概念化。该模型预测,高度支持性的出院干预措施将增强患者实施繁重自我护理的能力并避免再入院。
综合关于降低早期医院再入院率干预措施疗效的证据,并确定可能解释其不同效果的干预特征,包括这些干预措施对治疗负担以及患者出院后自我护理能力的影响。
我们检索了PubMed、Ovid MEDLINE、Ovid EMBASE、EBSCO CINAHL和Scopus(1990年至2013年4月1日),联系了专家并查阅了参考文献。
评估干预措施对因内科或外科病因住院超过24小时且出院回家的成年患者在出院后30天内全因或非计划再入院影响的随机试验。
评审员对提取试验特征,并使用基于活动的编码策略对干预措施进行特征描述;与作者确认了准确性。在对试验结果不知情的情况下,评审员根据累积复杂性模型记录干预措施在患者出院后给其增加额外工作的程度或支持其自我护理能力的程度。
出院后30天有或无院外死亡的全因或非计划再入院的相对风险。
在42项试验中,所测试的干预措施预防了早期再入院(合并随机效应相对风险,0.82[95%CI,0.73 - 0.91];P<0.001;I² = 31%),这一结果在各患者亚组中均一致。2002年之前发表的试验报告的干预措施比之后测试的干预措施有效1.6倍(交互作用P = 0.01)。在探索性亚组分析中,具有多个组成部分的干预措施(交互作用P = 0.001)、在护理提供中涉及更多个体的干预措施(交互作用P = 0.05)以及支持患者自我护理能力的干预措施(交互作用P = 0.04)分别比其他干预措施有效1.4倍、1.3倍和1.3倍。一个事后回归模型显示,为患者和护理人员提供全面的出院后支持具有增量价值。
所测试的干预措施在降低再入院率方面有效,但更有效的干预措施较为复杂且支持患者的自我护理能力。近期测试的干预措施效果较差。