Daphu Inderjit, Horn Sindre, Stieber Daniel, Varughese Jobin K, Spriet Endy, Dale Hege Avsnes, Skaftnesmo Kai Ove, Bjerkvig Rolf, Thorsen Frits
NorLux Neuro-Oncology Laboratory, Department of Biomedicine, University of Bergen, 5009 Bergen, Norway.
NorLux Neuro-Oncology Laboratory, the Luxembourg Public Research Center for Health, 1445 Strassen, Luxembourg.
Int J Mol Sci. 2014 May 16;15(5):8773-94. doi: 10.3390/ijms15058773.
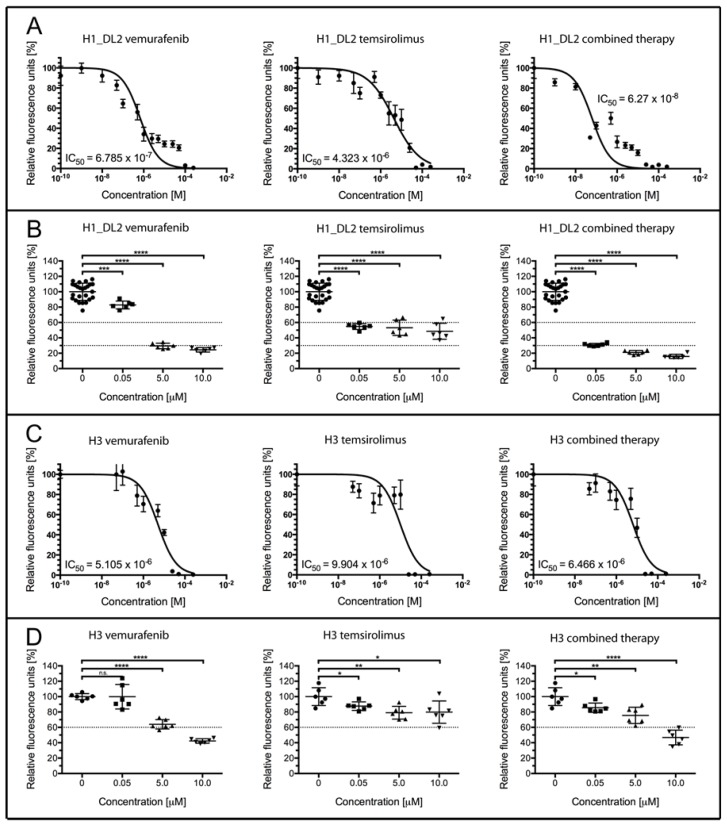
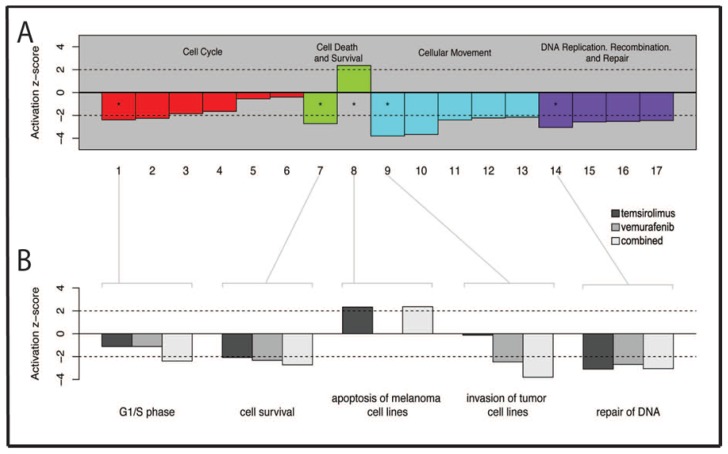
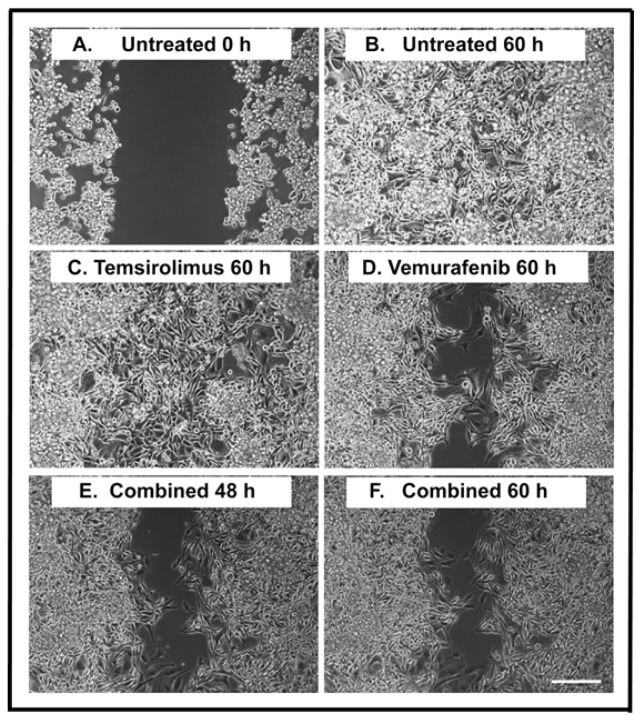
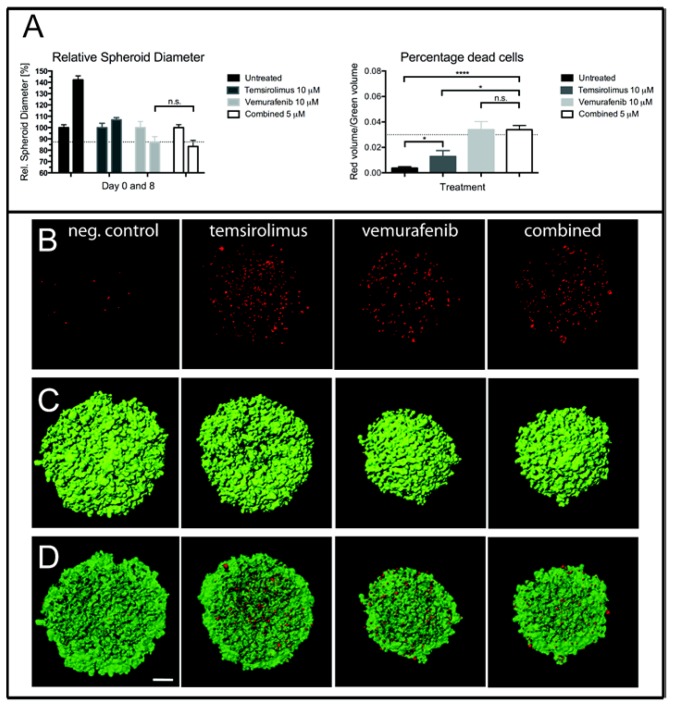
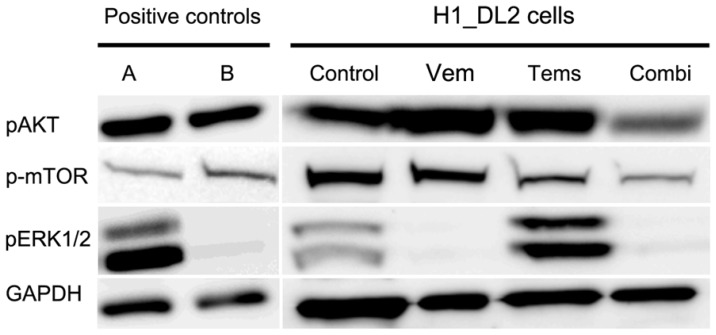
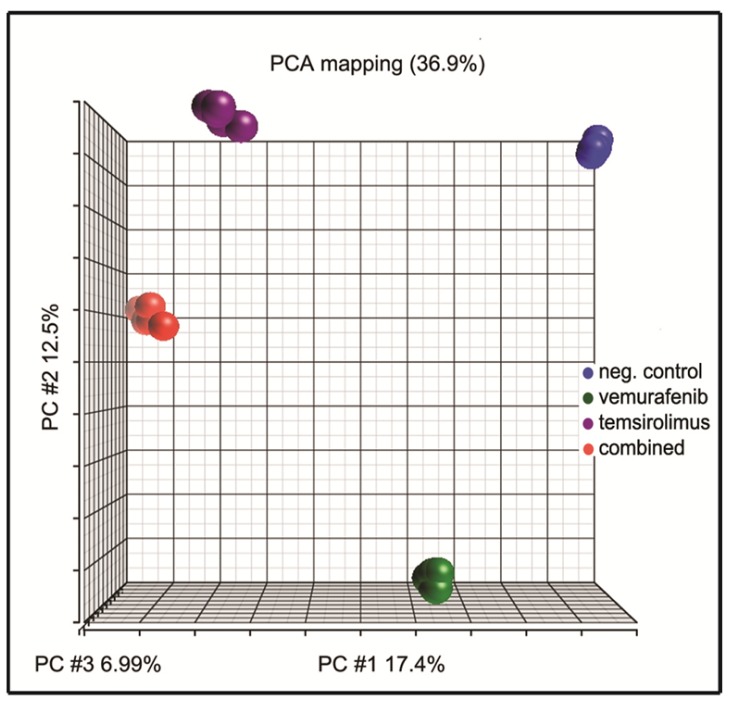
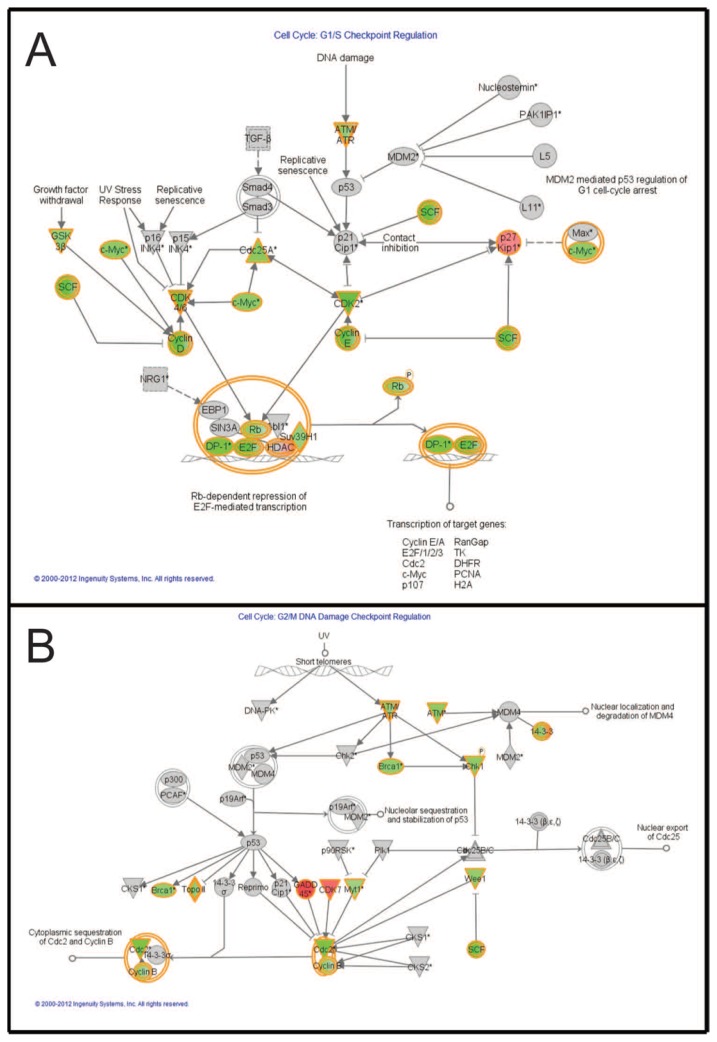
Malignant melanoma is the most lethal form of skin cancer, with a high propensity to metastasize to the brain. More than 60% of melanomas have the BRAFV600E mutation, which activates the mitogen-activated protein kinase (MAPK) pathway [1]. In addition, increased PI3K (phosphoinositide 3-kinase) pathway activity has been demonstrated, through the loss of activity of the tumor suppressor gene, PTEN [2]. Here, we treated two melanoma brain metastasis cell lines, H1_DL2, harboring a BRAFV600E mutation and PTEN loss, and H3, harboring WT (wild-type) BRAF and PTEN loss, with the MAPK (BRAF) inhibitor vemurafenib and the PI3K pathway associated mTOR inhibitor temsirolimus. Combined use of the drugs inhibited tumor cell growth and proliferation in vitro in H1_DL2 cells, compared to single drug treatment. Treatment was less effective in the H3 cells. Furthermore, a strong inhibitory effect on the viability of H1_DL2 cells, when grown as 3D multicellular spheroids, was seen. The treatment inhibited the expression of pERK1/2 and reduced the expression of pAKT and p-mTOR in H1_DL2 cells, confirming that the MAPK and PI3K pathways were inhibited after drug treatment. Microarray experiments followed by principal component analysis (PCA) mapping showed distinct gene clustering after treatment, and cell cycle checkpoint regulators were affected. Global gene analysis indicated that functions related to cell survival and invasion were influenced by combined treatment. In conclusion, we demonstrate for the first time that combined therapy with vemurafenib and temsirolimus is effective on melanoma brain metastasis cells in vitro. The presented results highlight the potential of combined treatment to overcome treatment resistance that may develop after vemurafenib treatment of melanomas.
恶性黑色素瘤是皮肤癌中最致命的一种,极易转移至脑部。超过60%的黑色素瘤具有BRAFV600E突变,该突变会激活丝裂原活化蛋白激酶(MAPK)通路[1]。此外,已证实通过肿瘤抑制基因PTEN活性丧失,PI3K(磷脂酰肌醇3激酶)通路活性增强[2]。在此,我们用MAPK(BRAF)抑制剂维莫非尼和PI3K通路相关的mTOR抑制剂替西罗莫司处理了两种黑色素瘤脑转移细胞系,即携带BRAFV600E突变且PTEN缺失的H1_DL2细胞系和携带野生型(WT)BRAF且PTEN缺失的H3细胞系。与单药治疗相比,联合使用这两种药物在体外抑制了H1_DL2细胞的肿瘤细胞生长和增殖。该治疗对H3细胞的效果较差。此外,当H1_DL2细胞生长为3D多细胞球体时,观察到对其活力有强烈的抑制作用。该治疗抑制了H1_DL2细胞中pERK1/2的表达,并降低了pAKT和p-mTOR的表达,证实药物治疗后MAPK和PI3K通路受到抑制。随后进行主成分分析(PCA)图谱的微阵列实验显示,治疗后有明显的基因聚类,且细胞周期检查点调节因子受到影响。全基因分析表明,联合治疗影响了与细胞存活和侵袭相关的功能。总之,我们首次证明维莫非尼和替西罗莫司联合治疗在体外对黑色素瘤脑转移细胞有效。所呈现的结果突出了联合治疗克服黑色素瘤维莫非尼治疗后可能出现的治疗耐药性的潜力。